Montefiore Einstein Cancer Center (MECC) was founded in 1971 and is celebrating its 50th year as a National Cancer Institute (NCI)-designated cancer center. Today, it draws on the skill and expertise of some 190 members. MECC’s overarching strategic priority is to better understand cancer and its causes in underrepresented groups. On the following pages, MECC Director Edward Chu, M.D., and four MECC members discuss what they are doing to detect, prevent, and treat cancer in the Bronx as well as nationwide.

We are enrolling up to 85% racial and ethnic minority patients into clinical trials, which is by far the highest percentage of any cancer center in the United States.
— Dr. Edward Chu
Dr. Chu has led National Cancer Institute (NCI)–designated Montefiore Einstein Cancer Center (MECC) since October 2020, after 10 years at the University of Pittsburgh Medical Center’s Hillman Cancer Center. In addition to holding the titles of vice president for cancer medicine at Montefiore Medicine and professor of medicine and of molecular pharmacology at Einstein, Dr. Chu is the Carol and Roger Einiger Professor of Cancer Medicine at Einstein.
You took the helm of the cancer center two years ago, and it’s now celebrating its 50th anniversary as an NCI-designated cancer center. What is your vision for the future?
Our cancer center was founded in 1971 and one year later received NCI designation—the fourth in the nation. We have long been recognized for our exceptional laboratory research and clinical care. My vision is to build upon that strong foundation to become the premier NCI Comprehensive Cancer Center in New York City and the nation for delivering personalized care to underserved communities facing heightened disparities in cancer and social determinants of health. How can we accomplish this? To start, our research is actively investigating the wide variation in the genomic ancestry of our community as well as the structural barriers to cancer care.
For more than 50 years our basic scientists have been making paradigm-shifting discoveries in the lab that have laid the groundwork for drug discovery and development. I’m pleased with our recent efforts to unify cancer research across Montefiore and Einstein. We have now strengthened our drug-discovery infrastructure and established a Phase 1 clinical trials initiative so we can more seamlessly bring these new therapies into the clinic. We are also focused on bringing the scientific rigor of our laboratory research to cancer care delivery to identify and overcome the hurdles that lead to worse outcomes for historically underrepresented groups. These efforts are particularly relevant to our Bronx population and will help us promote health equity in cancer care.
What is special about the Bronx in achieving your goals?
What makes us unique is that we serve one of the most diverse and socioeconomically disadvantaged communities in the country. The Bronx is New York’s only Hispanic-majority borough. Hispanics constitute about 55% of the population; another 30% of residents identify as Black or African American. Nearly one in three people in the Bronx was born in another country. And then there are the social determinants of health—such as education, housing, transportation, socioeconomic factors, and comorbidities—that challenge the delivery of cancer care as well as healthcare in general.
Black, African American, Hispanic, and other underrepresented groups historically have not participated in cancer research due to issues of trust in the scientific and medical communities. That applies to clinical trials and also to preclinical research, in which important molecular or genetic differences might be detected. We are tackling these challenges head-on so as to promote cancer health equity. Our patients must have access to the same type of cutting-edge clinical trials testing novel agents. Moreover, our scientists need to have access to tissue samples to better understand the biology of the main cancer types that affect our Bronx patients.
How can research in diverse populations help reduce disparities?
It’s critical. One of the main scientific priorities of our cancer center is to study the genomic, environmental, and behavioral factors that contribute to common cancers in the Bronx. Take prostate cancer. It is known to be much more aggressive in people who are Black or Hispanic than in whites, but it’s not exactly clear why. Our researchers are partnering with Johnson & Johnson to study molecular factors that contribute to the high rate of prostate cancer in these groups. They will also analyze the specific tumor antigens that trigger an immune response. This information will be especially helpful for developing novel immunotherapies such as cancer vaccines that are tailored to this population.
However, this is only one research project. In the past year alone, several of our investigators have been awarded grants to look into cancer disparities in the Bronx. An important and unique award is a “Stand Up to Cancer” grant that Bruce Rapkin [Ph.D., professor of epidemiology & population health and of family and social medicine at Einstein and co-leader, Cancer Epidemiology, Prevention and Control Program, and associate director, community outreach and engagement, at MECC] received to enhance the accrual of underrepresented groups into clinical trials, specifically addressing the issue of trust. Nationally, these groups account for only about 8% of cancer clinical trial participants. In sharp contrast, at our cancer center, we are enrolling up to 85% racial and ethnic minority patients into clinical trials, which is by far the highest percentage of any cancer center in the United States. Enrolling our patients in clinical trials not only helps them receive the latest treatments, but also provides valuable information as to whether these novel therapies are effective in diverse populations.
 Dr. Edward Chu at the Michael F. Price Center/Harold and Muriel Block Research Pavilion. (Photo by Karsten Moran)
Dr. Edward Chu at the Michael F. Price Center/Harold and Muriel Block Research Pavilion. (Photo by Karsten Moran)
What’s new about the way the cancer center is connecting with the Bronx community?
Montefiore has done a terrific job of providing a wide range of important services, free of charge, to people with cancer—from transportation assistance to meditation classes to nutritional support. Our cancer center is building on those efforts. We have established our own community advisory board. This group is partnering with us to conduct research in the community and to help us better communicate with and earn the trust of underrepresented groups that are skeptical of the healthcare system. We can’t just talk at people if we want to make change—they need to be an integral part of the conversation from the beginning. We’re learning, and we’re determined to do more.
Why is this interaction with the community so important?
We need to identify the key barriers to better care and do what we can to mitigate and eliminate them. For example, Black and Hispanic cancer patients are usually diagnosed at a later stage of disease than whites. There are multiple reasons for this—most importantly, the lower cancer-screening rates in underrepresented groups. This calls for research into new outreach strategies and population-specific, evidence-based interventions that can move the needle. The single most important action that anyone can take to prevent cancer is to follow the recommended screening guidelines.
Alyson Moadel-Robblee [Ph.D.] and Brendon Stiles [M.D.] recently received a LUNGevity Foundation grant to develop strategies to improve screening for early detection of lung cancer in our community. [Dr. Moadel-Robblee is professor of epidemiology & population health, of medicine, of radiation oncology, and of psychiatry and behavioral sciences at Einstein and deputy director of community engagement and cancer health equity at MECC. Dr. Stiles is professor of cardiothoracic & vascular surgery, of oncology, and of medicine at Einstein and associate director for surgical oncology at MECC]. Drs. Moadel-Robblee and Stiles are working with our community advisory board and other stakeholders to determine what strategies would be most effective—and then implement them in the Bronx.
You’ve recruited 42 new faculty. What has guided your choices?
Faculty recruitment has been one of my highest priorities, and we have been very strategic in this process. We’ve sought out truly exceptional research scientists and physicians who complement our existing strengths and add to the breadth and depth of our research. We have successfully recruited top specialists in the fields of lung cancer, hematologic malignancies, gastrointestinal cancer, cancer metastasis, and immunotherapy, as well as in the areas of epidemiology, cancer drug development, stem cell biology, and cell therapy. We have also placed a high priority on recruiting faculty committed to our social justice mission and focused on translating scientific discoveries into clinical practice.
Are there any current projects of note in translational research?
Yes, we have some great examples. The synTac fusion proteins developed by Steve Almo [Ph.D.] have the unique ability to target disease-specific T cells to fight cancer; they are now in preclinical and clinical testing for a variety of cancers. BRAF inhibitors target cancers driven by the mutated BRAF protein, and Evripidis Gavathiotis [Ph.D.] has developed some novel inhibitor molecules that show promise in treating leukemia, colon cancer, and melanoma. Xingxing Zang [Ph.D] has discovered several novel immune checkpoint pathways and has developed antibodies that target these pathways, including one now being tested in patients with advanced lung cancer who have failed standard treatment. [Dr. Almo is professor of biochemistry and of physiology & biophysics, the chair of biochemistry, and the Wollowick Family Foundation Chair in Multiple Sclerosis and Immunology at Einstein and co-leader of the Cancer Therapeutics Program at MECC. Dr. Gavathiotis is professor of biochemistry and of medicine at Einstein and a member of the Cancer Therapeutics Program at MECC. Dr. Zang is professor of microbiology & immunology, of oncology, of medicine, and of urology, and the Louis Goldstein Swan Chair in Women’s Cancer Research at Einstein and a member of Cancer Therapeutics Program at MECC.]

Localized cancer is highly treatable, but metastatic disease is not. Metastasis—the spread of cancer cells from a primary tumor to distant tissues or organs, where they form new, treatment-resistant tumors—accounts for the vast majority of cancer deaths. How do those cancer cells manage to evade therapy and persist undetected for many years—sometimes decades? Fortunately, researchers are now finding answers.
A leader in this fast-growing field of study is Julio Aguirre-Ghiso, Ph.D., endowed professor of cell biology, of oncology, and of medicine at Einstein, co-leader of the Tumor Microenvironment and Metastasis Program at Montefiore Einstein Cancer Center (MECC), the founding director of the new Cancer Dormancy and Tumor Microenvironment Institute at MECC, and co-director of the Gruss Lipper Biophotonics Center.
Dr. Aguirre-Ghiso was recruited from the Tisch Cancer Institute and Icahn School of Medicine at Mount Sinai, where he was an Endowed Mount Sinai Professor of Cancer Biology and co-leader of the Cancer Mechanisms Program at the Tisch Cancer Institute.
Dr. Aguirre-Ghiso’s metastasis studies are based on the observation that some cancer cells resist attacks from the immune system and cancer therapies by entering a long-term state of dormancy. They may not revive until much later, when surrounding conditions (the tumor microenvironment) change in ways that favor cell growth. Countless organisms, from bacteria to worms and bears, have evolved similar physiological adaptations for surviving in harsh environments.
Cancer-cell dormancy is not a new concept. The earliest known mention dates back to a 1934 monograph, The Spread of Tumours in the Human Body, by an Australian pathologist named Rupert A. Willis. However, his idea had little impact on researchers and even less on clinicians. Oncologists continued to focus on removing or destroying primary tumors in hopes of achieving a cure. Metastasis, if and when it did occur, was dealt with after the fact.
 Dr. Julio Aguirre-Ghiso at work with postdoctoral fellow Lornella Seeneevassen, left, and M.D./Ph.D. student Luis Valencia-Salazar, in his lab at the Michael F. Price Center. (Photos by Karsten Moran)
Dr. Julio Aguirre-Ghiso at work with postdoctoral fellow Lornella Seeneevassen, left, and M.D./Ph.D. student Luis Valencia-Salazar, in his lab at the Michael F. Price Center. (Photos by Karsten Moran)
Cancer dormancy came to Dr. Aguirre-Ghiso’s attention in the mid-1990s, when he was a doctoral candidate at the University of Buenos Aires, Argentina. “I kept hearing stories about cancer patients treated 15 or 20 years ago who were now relapsing. I was intrigued that the cancers had somehow stopped growing for a long time, although no one had a mechanism that could explain it,” he says. Finding that mechanism would become his life’s work.
Early on, Dr. Aguirre-Ghiso felt like a latter-day Don Quixote tilting at scientific windmills. “I would go to the annual AACR [American Association for Cancer Research] meetings and—among thousands of abstracts—mine would be the only one containing the keyword ‘dormancy,’” he says. “People argued that what I was seeing was an illusion—that cancer never pauses.”
But studies have since shown that cells from a variety of malignancies can escape from a primary tumor early in the course of the disease and then find a safe place to hibernate. While many of these disseminated cancer cells, or DCCs, remain dormant, others later awaken from their slumber and start proliferating and seeding secondary tumors.
Dr. Aguirre-Ghiso’s work has contributed significantly to this new view of metastasis. He discovered that cross-talk between DCCs and the tumor microenvironment regulates the cells’ ability to switch between dormancy and proliferation. His lab has provided key insights into the early spread of breast cancer and how that process leads to dormancy and to metastatic progression. He has also studied how intracellular signaling pathways adapt to enable cancer cells to survive during dormancy.
Treating cancer is like a chess game, and we kind of know the big moves that cancer is playing.
— Dr. Julio Aguirre-Ghiso
Dr. Aguirre-Ghiso is leveraging these insights to develop novel strategies for treating metastasis by maintaining DCC dormancy, killing dormant DCCs, or coaxing DCCs back into hibernation. An example of a tool to induce hibernation is an experimental drug called C26, the brainchild of Dr. Aguirre-Ghiso and Maria Soledad Sosa, Ph.D., of the Icahn School of Medicine at Mount Sinai, who trained with Dr. Aguirre-Ghiso.
In a 2015 study, the two investigators identified NR2F1, a receptor in tumor cell nuclei, as a master regulator of tumor cell dormancy. Building on this work, the team sifted through more than 100,000 chemicals to identify a compound that could activate this receptor and, ideally, make rapidly dividing cancer cells become dormant.
When tumor cells taken from patients with head and neck cancer were treated with that compound, known as C26, the cells could no longer multiply. Even more promising, C26 inhibited metastasis in mice injected with cells obtained from patients with highly aggressive head and neck cancer.
Drs. Aguirre-Ghiso and Sosa determined that C26, by activating NR2F1, pushes cancer cells into a prolonged dormancy by triggering a unique pattern of gene activity. Cancer patients whose tumor cells exhibit a similar gene-activity program tend to go longer without relapsing. This finding, published in the Journal of Experimental Medicine in 2021, suggested that C26 or similar drugs could be effective in inducing cancer-cell dormancy in patients and, ideally, keeping the cells dormant for a long time.
 From left, postdoctoral fellows Anna Adam Artigues and Rama Kadamb, Dr. Julio Aguirre-Ghiso, and Einstein instructor Deepak Singh. (Photo by Karsten Moran)
From left, postdoctoral fellows Anna Adam Artigues and Rama Kadamb, Dr. Julio Aguirre-Ghiso, and Einstein instructor Deepak Singh. (Photo by Karsten Moran)
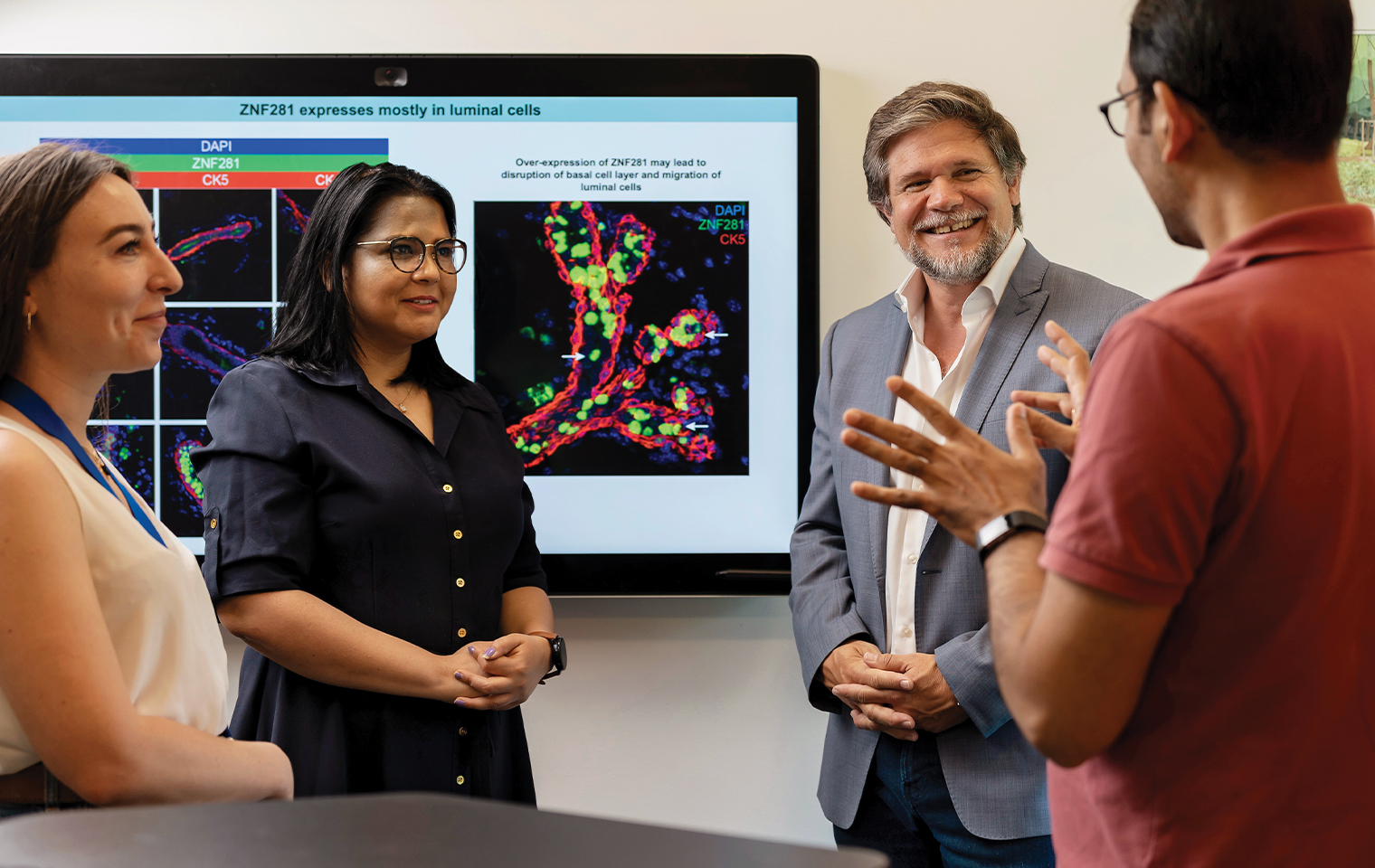
In a study published in 2022 in Nature Cancer involving a mouse model of breast cancer, Dr. Aguirre-Ghiso and colleagues reported that the expression of a transcription factor called ZFP281 locks early DCCs into a dormant state for very long periods, equivalent to 15 to 18 years in humans. The finding suggests that maintaining ZFP281’s expression in dormant DCCs could prevent cancer cells from reviving and becoming metastatic.
Interestingly, some subsets of these early DCCs upregulate NR2F1—raising the possibility that C26 could prolong dormancy in those cells while at the same time preventing any other dormant DCCs from reactivating and posing a danger.
“Skeptics have argued that by keeping DCCs alive and in place, we’re just creating a ticking time bomb that explodes if those dormant cells awaken,” says Dr. Aguirre-Ghiso. “I’d argue that all too often, current therapies allow cancer cells to revive because they ignore the importance of dormancy. We favor a rational, evidence-based therapeutic approach based on cancer-cell biology—which means turning on gene pathways that put DCCs to sleep.”
To test this treatment approach, Dr. Aguirre-Ghiso and his collaborators are conducting a clinical trial using azacytidine and retinoic acid (vitamin A) to reprogram metastatic prostate cancer cells into dormancy. The trial’s results should be available by early 2023.
Dr. Aguirre-Ghiso wants to do more than induce dormancy in DCCs; he also wants to eliminate them. In 2019, he co-founded a biotech startup called HiberCell to develop drugs to target and eliminate dormant DCCs. He is also working on tests to identify markers of cancer-cell dormancy, since such markers might allow cancer patients to be spared aggressive treatment with chemotherapy or radiation.
In another line of research, he is examining the relationship between aging and cancer dormancy. “We know that aging increases the risk of cancer,” he says, “and we’ve helped a group at Johns Hopkins show that aging also increases the risk of cancer relapse. Aging somehow makes DCCs in cancers such as melanoma more prone to reactivation. One of the reasons I came to Einstein was to collaborate with its experts on aging to learn more about this phenomenon.”
“Treating cancer is like a chess game, and we kind of know the big moves that cancer is playing. It has shown it can persist in a dormant state in many patients,” says Dr. Aguirre-Ghiso. “But as researchers and clinicians, we’ve traditionally responded to cancer’s opening gambit—its primary tumors—by countering with chemotherapy and radiation therapy instead of playing the long game: figuring out how to prolong lives by keeping disseminated cancer cells from causing metastases. The goal of my research is to develop treatments that are 10 steps ahead of what cancer tries to do.”

Whenever Yvonne Saenger gets frustrated with her research progress—as most investigators do from time to time—she recalls her years as a research fellow in the early 2000s.
“In those days, a diagnosis of stage 4 melanoma was a virtual death sentence, with the majority of patients surviving less than a year,” she says. “Today, thanks to immunotherapy, which primes the immune system to attack tumor cells, about 40% of those with advanced disease can expect to survive for five years. I just have to remind myself that we’ve made incredible progress—and that we can make even more.”
Dr. Saenger is associate professor of oncology, of microbiology & immunology, and of pathology at Einstein and a medical oncologist and co-leader of the Cancer Therapeutics Program at Montefiore Einstein Cancer Center (MECC).
Unlike many physicians, Dr. Saenger didn’t decide on a career in medicine until relatively later in her life. As a Harvard undergrad she majored in Russian literature, envisioning a life immersed in the fictional worlds of Tolstoy and Dostoevsky. However, an inner voice told her to pursue something with more social impact, leading her to enroll at Columbia University’s College of Physicians and Surgeons. Her life’s work came into focus when her younger sister was diagnosed with a rare type of skin lymphoma. “By then,” Dr. Saenger says, “I already knew I wanted to do immunology, but that pushed me more toward oncology.” (Her sister subsequently went into remission and continues to do well.)
Immunotherapy—a melding of immunology and oncology—appeared on Dr. Saenger’s radar in 2000, during her final year at Columbia. “I read about two researchers at Memorial Sloan Kettering Cancer Center [MSKCC] who were studying ways to activate the immune system to treat cancer,” she recalls.
Following an exchange of emails, the two researchers—Alan Houghton, M.D., and Jedd Wolchok, M.D., Ph.D.—invited Dr. Saenger to do a research elective at MSKCC. She returned there after her residency for a research fellowship. Working with these pioneering immunologists, she used a mouse model of metastatic melanoma to show that T-cell immunotherapies could be enhanced by simultaneously activating the animals’ B cells, the immune cells that produce antibodies. The findings were published in 2008 in Cancer Research, with Dr. Saenger as the lead author.
Like her mentors, Dr. Saenger is quick to respond to messages from medical students and young investigators. “The older you get, the more you realize that there’s only so much one human being can do,” she says. “Just as important as doing research is to inspire and encourage others to be more effective.”
Just a few years into her research career, Dr. Saenger was involved in arguably the most important advance in cancer treatment in generations. While at MSKCC, she participated in the early clinical trials of the immunotherapy drug ipilimumab (Yervoy), the first medicine ever to improve overall survival in patients with melanoma.
“I remember when some of our patients’ hair began to turn white—a sign that the medicine was working as intended,” Dr. Saenger says. “Melanoma develops in the melanocytes, the cells that produce the pigment melanin. At the same time ipilimumab was destroying the melanocytes within their tumors, it was also destroying the melanocytes that give hair its color. It was exciting to witness, like something out of science fiction.” The Food and Drug Administration approved ipilimumab for treating melanoma in 2011.
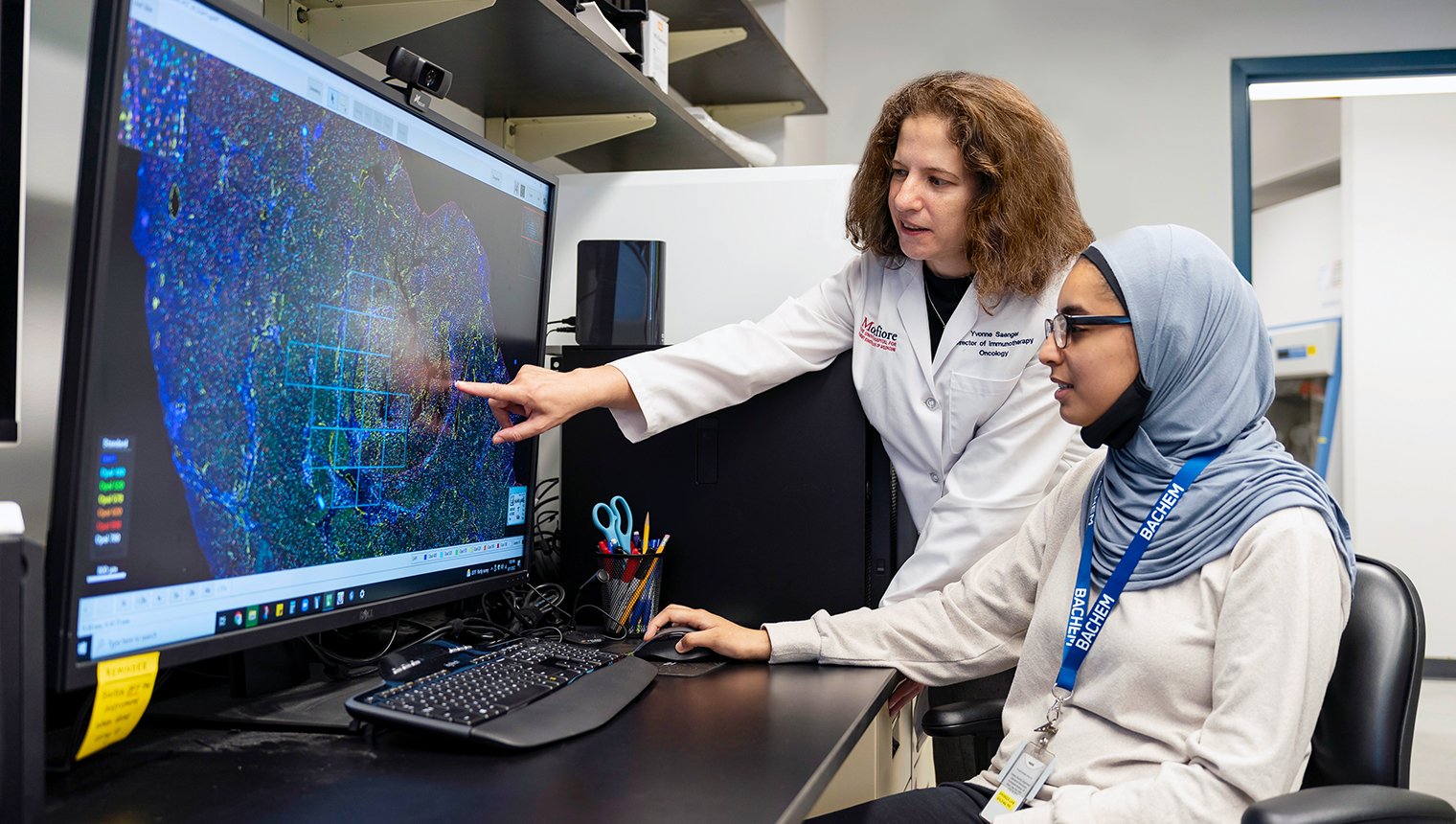 Dr. Yvonne Saenger, above left, works with Einstein research technician Sharmin Sultana at the Montefiore Einstein Cancer Center’s Immune Monitoring Core. (Photo by Karsten Moran)
Dr. Yvonne Saenger, above left, works with Einstein research technician Sharmin Sultana at the Montefiore Einstein Cancer Center’s Immune Monitoring Core. (Photo by Karsten Moran)
Dr. Saenger came to Einstein in 2021 after leading her own labs at the Icahn School of Medicine at Mount Sinai and then at Columbia. Today, she is developing prognostic biomarkers at MECC for patients with aggressive (stage 2 or 3) melanoma.
In stage 2 melanoma, the cancer is no longer confined to the outer skin layer but has not spread to nearby skin or lymph tissue. In stage 3, the cancer has spread to nearby skin or lymph tissue but not to other parts of the body. Patients in both stages face a 50% risk of tumor recurrence, but predicting recurrence is difficult using traditional tissue-examination techniques.
“Immunotherapy can help prevent recurrence but also can have potentially serious complications,” she explains. “We don’t want to subject low-risk patients to such hazards, nor do we want to withhold treatment from anyone who might benefit. We need better prognostic tests so we can personalize immunotherapy.”
One of her promising biomarkers is based on a study she published in 2014 in the Journal of Investigative Dermatology involving patients with aggressive melanoma. Dr. Saenger found that the elevated expression of 53 immune-related genes correlated with better postsurgical outcomes in the patients.
That 2014 study assessed the accuracy of the 53-gene panel on tissue samples from 48 melanoma patients. Now, in a study funded by the National Institutes of Health (NIH), she and her colleagues at other centers are more rigorously evaluating the 53-gene panel on a much larger set of tissue samples—a critical step toward readying it for clinical use.
Under a separate NIH grant, Dr. Saenger is developing a “pathomics biosignature” to further fine-tune treatment decisions for the same patient population.
“We’ve known for decades that the immune system limits the progression of melanoma, and that higher levels of tumor-infiltrating lymphocytes portend a favorable outcome,” she notes. “However, the way that pathologists analyze those lymphocytes is somewhat subjective, and the results can vary widely from pathologist to pathologist.”
To bring infiltrating-lymphocyte analysis into the computer age, Dr. Saenger’s team has developed three different digital pathology methods to estimate the risk of melanoma recurrence. Each method provides unique information about the lymphocytes and the tumor immune microenvironment. “By combining these methods, and using the 53-gene panel, we hope to identify those patients whose immune systems are so good that we don’t have to expose them to immunotherapy, with its considerable risks, such as autoimmune disease, and its considerable expense as well,” she says.

The precipitous decline in colorectal cancer in the United States is one of oncology’s great successes. Since 1975, this overall incidence has fallen by 37%, with the mortality rate tumbling by 50%. Most of the credit goes to early screening and improved treatment—but a dark cloud hangs over those sunny statistics.
“In the United States and other affluent countries, the incidence of this cancer among young adults [those under age 50] has risen 63% since 1988,” says Peter T. Campbell, Ph.D., professor of epidemiology & population health at Einstein and a member of the Cancer Epidemiology, Prevention, and Control Program at Montefiore Einstein Cancer Center (MECC). “Not only that, but early-onset colorectal cancer tends to be diagnosed at later stages and is particularly aggressive.”
Inherited genetic diseases, such as Lynch syndrome, can explain some of those cases. But the cause of at least half of colorectal cancers in younger people remains a mystery. Increases in obesity, changes in diet, and new environmental exposures may be to blame. Of note, Black and Hispanic men, in the Bronx and nationally, are diagnosed with early-onset colorectal cancer at a higher rate than their white counterparts and are more likely to die of the disease.
In 2020, the National Center for Health Statistics reported that there were 17,930 cases of early-onset colorectal cancer, with 3,640 deaths (accounting for 10% of all colorectal cancer fatalities). Researchers estimate that the incidence of early-onset colorectal cancer will rise by more than 140% by 2030.
Numerous studies have looked at early-onset colorectal cancer, but most have been too small to provide conclusive data. Taking a more expansive view, Dr. Campbell leads a major new study called the Colorectal Cancer Pooling Project (C2P2), which aims to better understand the risk factors for early-onset colorectal cancer. C2P2 combines data from 25 prospective cohort studies being conducted in North America, Europe, and Asia. It was started under the auspices of the National Cancer Institute Cohort Consortium, which helps create large-scale collaborations to tackle important scientific questions about cancer and quicken the pace of research.
I wanted to learn more about cancer prevention in the context of systemic racism.
— Dr. Peter Campbell
Dr. Campbell’s path to epidemiology was unusual. He started in kinesiology, the scientific study of human movement, earning both bachelor’s and master’s degrees in the field, with a stint as a swim coach in between. During his graduate studies, at Toronto’s York University, he worked with Peter Katzmarzyk, Ph.D., a kinesiologist who specializes in pediatric obesity and diabetes. “That was the beginning of my shift from human performance to human health—from the individual to populations,” Dr. Campbell says.
He went on to earn a Ph.D. in epidemiology at the University of Toronto in 2006, with a focus on colorectal cancer, following the lead of his mentor, John R. McLaughlin, Ph.D. “It was a good fit with my background in exercise science, since there was emerging evidence that physical inactivity and metabolic imbalances were major risk factors for this disease,” Dr. Campbell says.
After earning a postdoc at the Fred Hutchinson Cancer Center in Seattle and then working as a senior investigator at the American Cancer Society (ACS) in Atlanta, he expanded his focus to include early-onset colorectal cancer. “Back then, researchers said it had to be caused by obesity,” says Dr. Campbell. “But it has since become clear that the development of early-onset colorectal cancer is multifactorial, likely involving dozens of environmental influences on top of hundreds of genetic variants that can make you more susceptible to this cancer. Only a large study, such as C2P2, can begin to unravel the causes of early-onset colorectal cancer and to identify the ones we have to pay the most attention to.”
Dr. Campbell came from the ACS to Einstein in 2021. “I wanted to learn more about cancer prevention in the context of systemic racism and its possible biological effects on certain racial and ethnic groups in the Bronx,” he says. “So Einstein seemed like it would be a really good fit for me.”
C2P2’s 25 prospective studies are providing detailed demographic, clinical, pathological, and epidemiological data on some 3.7 million people. “We expect to have data on more than 3,000 patients with early-onset colorectal cancer—about 30 times the size of any study published thus far,” Dr. Campbell says. “So the data should be quite robust.”
C2P2 is looking at the relative roles played by lifestyle and behavioral risk factors, including the usual colorectal cancer suspects, such as body mass index, diet (e.g., red-meat intake), smoking, and alcohol use. The study will also assess novel risk factors (such as antibiotic use, allergies, and sleep) that have turned up in smaller studies. Finally, the study will look at contributions of nonmodifiable risk factors, such as family history of colorectal cancer, diabetes, and inflammatory bowel disease.
“In terms of risk factors, I think early-onset disease will look a lot like late-onset disease,” he says. “But I expect the C2P2 study will find some different risk factors for early-onset disease that can help reveal which young adults would benefit the most from screening and at what age. Ideally, the study will also reveal biomarkers for identifying and screening at-risk young adults. In turn, we hope those blood-based markers point to factors that can be changed via lifestyle or environmental modification.”
Studies clearly show that screening for colorectal cancer saves lives by catching the disease early, when it’s much more treatable. “Unfortunately, our healthcare system doesn’t have the resources for mass screening. Even if we did, I’m not sure we could convince many young people—those below the recommended age of 45—to undergo colonoscopies. It would be much more compelling if we could say to select individuals, ‘You’re at especially high risk; you need to be tested,’ or ‘You need to modify these behaviors to reduce your risk of disease.’”
Dr. Campbell emphasizes that future epidemiology studies of colorectal cancer that he and colleagues are planning must include more nonwhite participants—especially from groups known to be at increased risk from the disease.
“Here in the Bronx, for example, the incidence of colorectal cancer among Blacks is about the same as the national average, but their mortality rate here is 20% higher,” he says. “Economic disparities and less access to care probably have something to do with it. But their disease could differ at a biological level and might require looking at different risk factors or biomarkers or administering different treatments.”

It pays to be curious. In search of seeds to grow in her basement for a science fair project, 14-year-old Srilakshmi Raj and her father dialed the lab of Frederick Ausubel, Ph.D., at Harvard Medical School, fully expecting that this world-renowned geneticist would take a call from a young budding scientist. As it turned out, a friendly postdoctoral fellow answered the phone and said, “You can’t do a proper experiment in your basement—why don’t you use our greenhouse?” Srilakshmi—who goes by Sri (pronounced “Shree”)—accepted the offer and completed her science project, which compared how plants of the same species but different original localities (ecotypes from Siberia and America) responded to vernalization (the induction of flowering by exposure to prolonged cold). She won first place at the Massachusetts state science fair.
Months later, when the postdoc needed a research assistant during her maternity leave, she asked Sri to take on the responsibility of contributing to Dr. Ausubel’s studies. Sri stayed on to work there for two and a half years.
“This was my introduction to the idea that genetic differences shape our response to the environment, and it has permeated my research ever since,” says Dr. Raj, who in 2012 earned a doctorate in biological anthropology at Cambridge University in England. She is now assistant professor of population genetics at Einstein and a member of the Cancer Epidemiology, Prevention, and Control Program at Montefiore Einstein Cancer Center (MECC).
Dr. Raj has already studied a surprising variety of topics in her career, including how variations in genes, diet, and environment affect type 2 diabetes and obesity among Asians; how genetic variations among immunity-related interleukin genes may influence disease risk in a range of populations; and risk factors for childhood growth stunting in India.
“The same basic tool kit can be used in almost any research setting where genetic and environmental factors are at play,” she explains—a tool kit containing a trio of disciplines:
With most complex diseases, the rule of thumb is that just 30% of the cause is genetic, so we have to look at the bigger picture.
— Dr. Srilakshmi Raj
Dr. Raj was recruited by MECC and joined the Einstein genetics department in late 2021, and she uses those disciplines to study the origins and distribution of cancer and other complex conditions in the Bronx.
“Most genetic studies have been carried out in whites of Northern European descent, but the Bronx has a mosaic of human populations with only 9% European whites,” she says. “We need to better understand the genetic risk factors for disease in different populations and to learn how they interact with their local urban environments to influence disease risk.”
Dr. Raj’s initial studies focused on colorectal cancer, which has a higher incidence among African Americans. “Not only is their risk 20% to 30% higher than that of European populations but they also tend to be diagnosed with colorectal cancer at a younger age, and their disease is more aggressive,” she says. “This cancer is what led to the untimely death of the actor Chadwick Boseman, among so many others.”
Dr. Raj notes the low rate of cancer screening in historically marginalized communities—one of the many health disparities affecting people from these communities. “Among other efforts, we clearly need to encourage screening in these groups,” she says, “but population genetics also has a role to play here. We can use ancestry-based genomic information to identify distinct risk profiles among different populations so we can predict and treat illness more effectively.”
When patients walk into a clinic, Dr. Raj says, “they typically check off a box that they’re Black or Hispanic, and so on—which doesn’t hold any genetic weight. ‘Black’ could mean African American, West Indian, Brazilian, or Cuban, or a mixture of different ancestries. Using population genetics, we can go beyond broad racial categories to better define the various populations in the Bronx and each group’s risk profiles for cancer and other diseases, with the goal of developing more-targeted therapies.”
“Since genes don’t operate in a vacuum, we also need to ask how they interact with different environmental, societal, and cultural factors—diet and exercise, for example—to influence disease risk and health outcomes,” says Dr. Raj. “With most complex diseases, the rule of thumb is that just 30% of the cause is genetic, so we have to look at the bigger picture—and this is where I put my anthropologist hat on.”
In her work on childhood stunting, she recalls, “I spent a lot of time in the rain forests and deserts of India, trying to understand how those environments contribute to differences in complex disease outcomes. For my current work in the Bronx, I hope to get out of the lab and engage directly with the local community.”
Ideally, all this genetic and environmental information will eventually find its way into Montefiore’s electronic health record system, giving a clearer picture of patients’ disease risk and helping physicians prescribe personalized treatments.
Dr. Raj’s appetite for scientific inquiry has already led to several collaborations around Einstein. She works with Parvathi Myer, M.D., assistant professor of medicine at Einstein and a physician at Montefiore, on studies of colorectal cancer risk in individuals of African ancestry, and with John Greally, Ph.D., D.Med., professor and chief of genomics in the department of genetics, to study the relationship between genetic and epigenetic variation in global populations. She is also sowing the seeds for future projects with other cancer center members.
“The underlying theme of my work is that one size does not fit all,” she says. “One treatment might help some people but might not work for others. We can use genetics to better understand disease risk and find treatments that serve larger segments of the community.”