Moving basic-science discoveries out of the lab and into clinical trials isn’t easy. Just ask Steven Almo, Ph.D., professor and chair of biochemistry at Einstein. In 2011, he came up with an idea for a new form of immunotherapy, known as Immuno-STAT™, that didn’t enter clinical trials until 2019.
Thanks to grant support from the National Institutes of Health, he and his Einstein colleagues were able to develop Immuno-STAT into a potential therapy against cancer as well as autoimmune diseases. But then came a major hurdle. “We were confronting the ‘Valley of Death,’” says Dr. Almo—the term describing the gap between invention and commercial application, where lack of funding dooms many advances.
“There’s no shortage of scientists with good ideas for new drug technologies,” continues Dr. Almo, who is also a professor of physiology and biophysics, a co-leader of the Cancer Therapeutics Program at Montefiore Einstein Cancer Center, the Wollowick Family Foundation Chair in Multiple Sclerosis and Immunology, and the director of the Einstein Macromolecular Therapeutics Developmental Facility.
“In our case, we were fortunate that Einstein’s office of biotechnology and business development understood what our innovative science could mean to patients,” Dr. Almo says. “It relentlessly pursued finding a licensing partner that could raise the funding needed to further develop our technology and bring it to clinical trials.”
Janis Paradiso, M.B.A., directs Einstein’s office of biotechnology and business development. “Our challenge in advancing a drug discovery is finding a champion—typically a biotechnology company, a life-sciences entrepreneur, or a venture capital firm—that believes in it and has the resources to develop it,” she says.
“That partner then licenses our IP [intellectual property], hoping its investment will culminate in a drug approved by the U.S. Food and Drug Administration [FDA],” she adds. “The licensing agreement allows us to hold the licensing partner’s feet to the fire to ensure that the drug’s development is being advanced in a diligent manner.”
Over the past year, Ms. Paradiso says, Einstein has gone from having two IP assets in clinical trials to four—with more in the works. “It’s an exciting time,” she says.
Here, we interview the four Einstein researchers whose drug discoveries are currently in clinical trials and look into what their approval could mean for patients.
Since 1976, some two dozen ebolavirus disease outbreaks, involving several different ebolavirus strains, are known to have occurred in Africa. The largest outbreak in recorded history—the 2013–16 Western African epidemic—killed more than 11,000 people and was caused by the Zaire strain.
The good news is that monoclonal antibodies, which bind to and neutralize specific pathogens, have emerged as successful treatments for Ebola patients. The FDA approved two monoclonal-antibody therapies in late 2020. However, they’re effective against only the Zaire strain and not the other two ebolavirus strains, Sudan virus and Bundibugyo virus, which have also caused major outbreaks. One of those strains—Sudan virus—was responsible for the recent ebolavirus outbreak in Uganda that killed 55 people.
“The sub-Saharan region of Africa is a hot spot for these viruses,” says Kartik Chandran, Ph.D., professor of microbiology & immunology, the Gertrude and David Feinson Chair in Medicine, and the Harold and Muriel Block Faculty Scholar in Virology at Einstein. He lists other strains that have appeared in the area, in addition to the three major disease-causing ebolaviruses: the Taï Forest ebolavirus is known to have infected one person, the Reston strain infects nonhuman primates, and the Bombali ebolavirus has been isolated from bats.
“The development of ebolavirus therapies has proceeded slowly, in fits and starts, with most research sponsored by the U.S. Department of Health and Human Services and the Department of Defense,” Dr. Chandran says. “Without the funding and the time to develop separate drugs for each strain of ebolavirus, we and others realized we needed a pan-ebolavirus drug that could treat or prevent infection caused by any of them.”
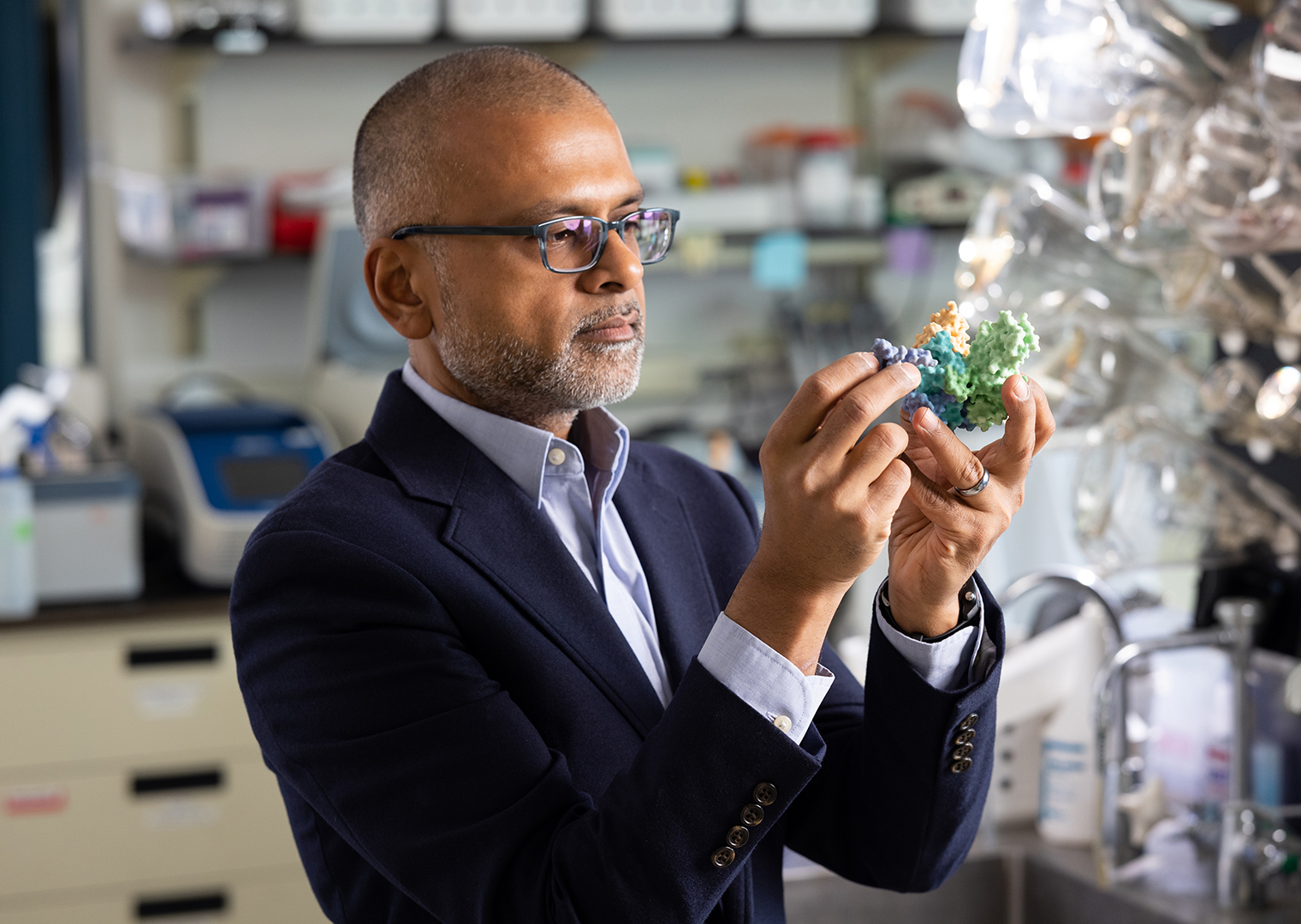 Kartik Chandran, Ph.D., examines a molecular model of the Ebola spike protein. (Photo by Jason Torres)
Kartik Chandran, Ph.D., examines a molecular model of the Ebola spike protein. (Photo by Jason Torres)
The search for such a drug began in 2016. Dr. Chandran—along with colleagues from the U.S. Army Medical Research Institute of Infectious Diseases and the biotech companies Adimab and Mapp Biopharmaceutical—sifted through the antibodies from a survivor of the 2013–16 Zaire ebolavirus epidemic, looking for antibodies that recognized other ebolaviruses too.
Out of 349 different antibodies tested, the researchers identified one that could neutralize the three major Ebola strains that infect humans. “We call it the ‘rainbow unicorn’ antibody,” Dr. Chandran says. A second antibody from the same ebolavirus survivor showed promise, but it required some fine-tuning in the lab.
“Antibodies that work against ebolavirus do so by attaching to spike proteins on the viral surface that the microbe needs to penetrate and infect cells,” Dr. Chandran explains. “Thanks to our consortium’s molecular engineering skills, we were able to modify the second antibody’s structure into a sort of skeleton key that fits onto and blocks multiple spikes.”
Lab tests showed that the two monoclonal antibodies combined were able to neutralize all known ebolavirus strains by successfully attaching to their spike proteins. Then, in proof-of-concept animal studies, the two-antibody combination, dubbed MBP134, was administered to macaque monkeys that had been infected with normally fatal doses of ebolavirus. “The antibody combination proved to be almost completely protective for the virus-infected monkeys,” Dr. Chandran said.
MBP134 is being evaluated in a phase 1 clinical trial, and preliminary results indicate that the therapy is safe for humans. However, since Ebola outbreaks are relatively rare and unpredictable, a conventional phase 2/3 trial to evaluate the drug cocktail’s effectiveness in patients isn’t possible. Nevertheless, says Dr. Chandran, physicians in Uganda are giving the drug to a handful of patients infected in the ongoing Ebola outbreak in Sudan, under the FDA’s compassionate-use protocol allowing unapproved drugs when no other treatments are available.
Mapp Biopharmaceutical and the federal government’s Biomedical Advanced Research and Development Authority recently announced a contract to further develop MBP134 into an FDA-approved drug. Dr. Chandran hopes that thousands of doses of MBP134 will be stockpiled before the next outbreak. “Lives depend on our being able to deploy it quickly,” he says.
If you had wandered into Einstein’s Falk Center seven years ago, you might have overhead Joel Friedman, M.D., Ph.D.—a regular in the gym’s noontime pickup basketball games—extolling the virtues of curcumin, a derivative of the gold-colored herb turmeric.
“I hadn’t been able to play basketball for several months because my knees hurt so much from osteoarthritis,” recalls Dr. Friedman, professor of microbiology & immunology and of medicine at Einstein. “My orthopedist had nothing to offer except suggesting I take up shuffleboard instead.” But then a postdoctoral student in Dr. Friedman’s lab told him that his grandfather, a healer in India, applied a mixture of curcumin and coconut oil to aching joints. The remedy seemed to make sense: Dr. Friedman found hundreds of papers published on the health benefits of curcumin, most notably its anti-inflammatory quality.
“After I started applying curcumin plus coconut oil to my knees—voilà!—I was able to play basketball again and resume doing Chinese martial arts,” he recalls. “It made me think that curcumin might have real potential as an osteoarthritis drug. But as I read the studies exploring curcumin as a therapy, I realized that they’d all hit the same wall: No matter how much curcumin you ingest with pills, or how much you rub on your skin, the body doesn’t absorb it too well.”
 Joel Friedman, M.D., Ph.D., has developed a topical arthritis drug. (Photo by Jason Torres)
Joel Friedman, M.D., Ph.D., has developed a topical arthritis drug. (Photo by Jason Torres)
Studying the yellow curcumin concoction in his lab, Dr. Friedman discovered that fatty acids in coconut oil transported only small amounts of curcumin through the skin and into the joint. What was needed, he realized, was a third ingredient: a solvent capable of dissolving high concentrations of curcumin and its fatty-acid carrier. Finding one proved quite a challenge, since nearly all good solvents for curcumin aren’t safe to use. Finally—after a period of testing and aided by his previous research on nanoparticles—he arrived at a formula for safely delivering an effective dose of curcumin through the skin.
Dr. Friedman connected with entrepreneurs, who formed Vascarta, a company that licensed the technology from Einstein with the goal of developing it into a drug. A safe and effective topical drug for joint pain could be a boon for the 31 million Americans who suffer from osteoarthritis, the most common disability among adults. Many of them rely on oral nonsteroidal anti-inflammatory drugs (NSAIDs), which can cause serious side effects. Diclofenac, the only topical FDA-approved drug for arthritis pain, is also an NSAID; for safety reasons, the name-brand drug Voltaren and other topical diclofenac products should not be applied for more than 21 days.
Curcumin triggers tissues to produce the signaling molecule nitric oxide, which may be a magic bullet for a number of conditions.
— Dr. Joel Friedman
So far, Dr. Friedman’s curcumin compound has been patented and has progressed through animal studies and a phase 1 trial in India to assess safety. A phase 2 trial involving osteoarthritis patients is being planned. Although reduced joint pain would be the trial’s primary outcome, Dr. Friedman believes his compound’s benefits may extend beyond the joints: The preclinical studies, he says, detected curcumin in the bloodstream after the product was topically applied.
“Curcumin triggers tissues to produce the signaling molecule nitric oxide, which may be a magic bullet for a number of conditions,” says Dr. Friedman. “One of nitric oxide’s best-known effects is vasodilation, which suggests that boosting nitric oxide levels via curcumin could potentially lower blood pressure and treat systemic problems caused by sickle-cell disease.” He also points to studies suggesting that nitric oxide may reduce systemic inflammation, a contributor to heart disease, cancer, and diabetes as well as arthritis.
“I have no doubt that prescription drugs based on curcumin will one day make it to the market,” Dr. Friedman says. “We hope to get our product there first.”
Sprouting from T cells and other immune cells are proteins called “checkpoint” receptors. When they make contact with proteins in the body’s own cells, the interaction prevents a possible autoimmune reaction. Diabolically, most types of cancer cells express proteins and other molecules aimed at inactivating T cells by binding to their checkpoint receptors.
In the illustration above, a tumor cell (at left) has deployed three different molecules to inactivate a T cell (at right) by stimulating its Tim-3 checkpoint receptors (purple). Two of the tumor molecules are the secreted proteins galectin-9 and HMGB-1 (blue and yellow); the third is phosphotidylserine (green), a cell-surface phospholipid.
The immune-checkpoint inhibitor TQB2618, now in clinical trials against several types of cancer, stops tumor molecules from shutting down T cells. The illustration shows that TQB2618 molecules (pink) have bound to the T cell’s purple Tim-3 receptors, thereby preventing any of the tumor molecules from doing so. Protected from inactivation, the T cell can now attack cancers.
Xingxing Zang, M.Med., Ph.D., develops immune-checkpoint inhibitors (ICIs)—monoclonal antibodies that unleash the full power of the immune system to attack a wide range of human cancers. “Unlike surgery, radiation, and chemotherapy, ICIs are immunotherapies, meaning they enlist the body’s own immune system to attack tumors,” says Dr. Zang. “It is the future—a completely different approach to cancer treatment.”
Dr. Zang has already patented more than 10 ICIs, most of which have been licensed by biotechnology companies for further development. One of his ICIs is now being evaluated in clinical trials in China. Dr. Zang has also launched three start-up companies in the United States and Israel to develop early drug prototypes. “He keeps our office busy,” Ms. Paradiso says.
Dr. Zang is a professor in the departments of microbiology & immunology, oncology, medicine, and urology and the Louis Goldstein Swan Chair in Women’s Cancer Research at Einstein, and a member of the National Cancer Institute–designated Montefiore Einstein Cancer Center. His postdoctoral mentor, James P. Allison, Ph.D., shared the 2018 Nobel Prize in Physiology or Medicine for coming up with the idea for ICIs and developed Yervoy, the first of nine ICIs now on the market.
Today’s ICIs have succeeded against cancers that once were intractable. Previously, for example, patients with metastatic melanoma lived an average of only seven months following diagnosis; now, some melanoma patients treated with ICIs have survived for more than a decade. “But the problem,” explains Dr. Zang, “is that whether we are talking about melanoma or other cancers for which ICIs are prescribed, the majority of patients don’t respond to these drugs.”
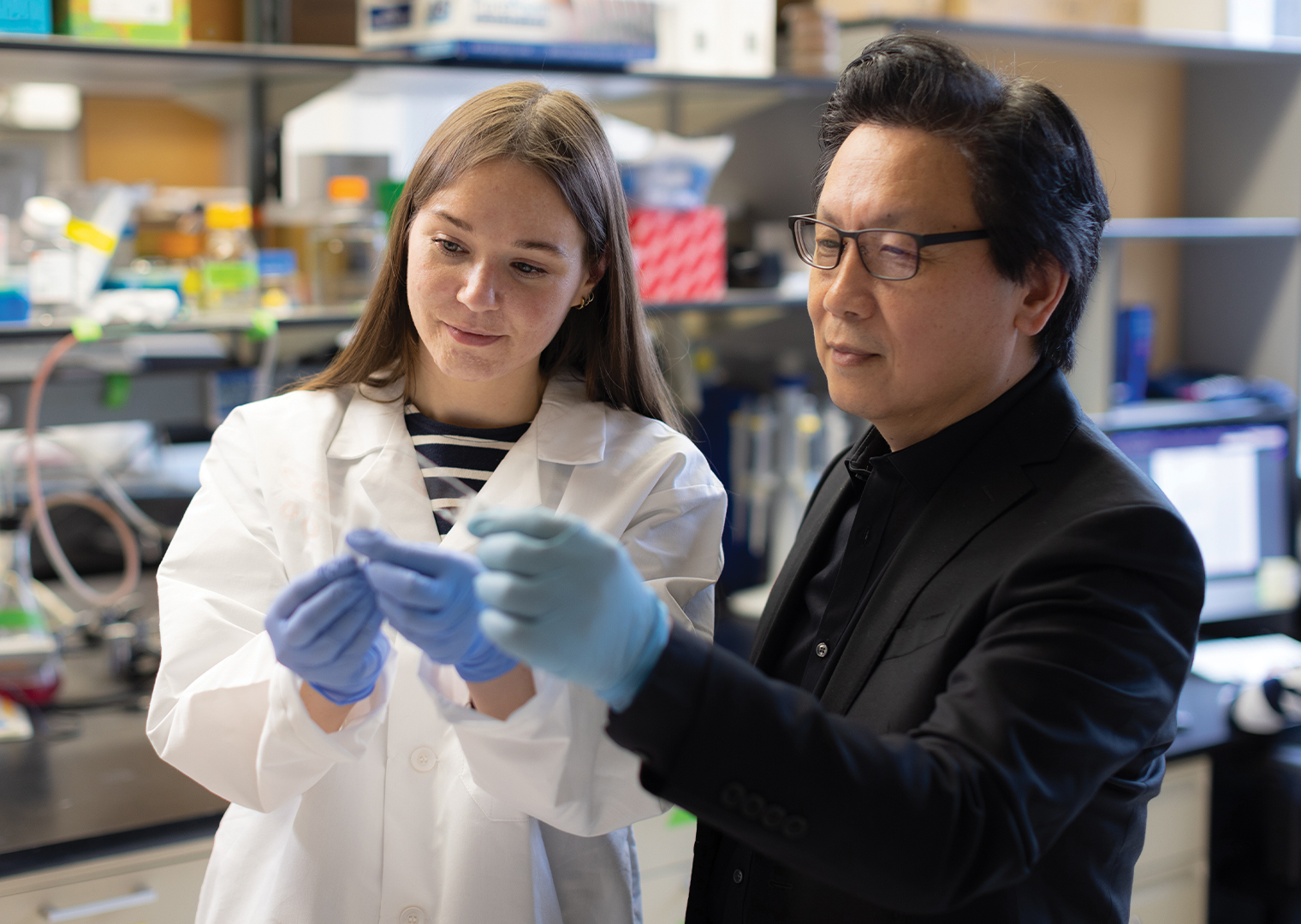 Xingxing Zang, M.Med., Ph.D., works with postdoctoral fellow Anne Madsen, Ph.D. (Photo by Jason Torres)
Xingxing Zang, M.Med., Ph.D., works with postdoctoral fellow Anne Madsen, Ph.D. (Photo by Jason Torres)
Dr. Zang excels at discovering checkpoints that the current ICIs don’t target—discoveries that have led to new ICIs that may work where others have failed. “I want to do as much as I can to bring novel and better drugs to patients,” he says.
The first of Dr. Zang’s cancer-fighting ICIs to make it to clinical trials is a monoclonal antibody called TQB2618, which binds to the T-cell checkpoint receptor known as Tim-3. By binding to the Tim-3 receptor, the antibody “locks out” three different molecules that tumor cells deploy to bind to Tim-3 and put the brakes on T-cell activity. (See illustration above.) A leading Chinese drug company, the Chia Tai Tianqing Pharmaceutical Group, is sponsoring several trials of TQB2618 in China.
A phase 1 trial of TQB2618 demonstrated its safety in advanced cancer patients in 2021. Now seven new clinical trials are studying the drug in various types of cancer, including both solid cancers and blood cancers:
Early in 2023, another of Dr. Zang’s ICIs, the first of its kind, will begin a phase 1 trial in the United States for the treatment of several types of solid tumors. The trial is sponsored by NextPoint Therapeutics in Cambridge, Mass., of which Dr. Zang is the scientific co-founder.
“I’m hopeful that in a decade, checkpoint inhibitors will have become a standard treatment for many forms of cancer,” Dr. Zang says.
Anticancer Immuno-STAT proteins are designed to selectively activate “disease-relevant” T cells, avoiding the generalized, life-threatening T-cell reactions that other drugs can trigger. Immuno-STAT CUE-101, pictured here, rallies T cells to attack recurrent metastatic head and neck cancers caused by human papilloma virus (HPV) 16. Such a tumor (bottom of illustration) displays antigenic fragments of HPV 16’s E7 protein (red) and can be recognized by T cells possessing receptors for the E7 protein (green). To find those specific T cells, CUE-101 molecules have two “targeting arms” (blue); each arm is equipped with E7 protein fragments (red) that enable CUE-101 to preferentially bind T cells (see large cell at center) that have E7-specific receptors. Then CUE-101’s “activating arms”—each with two copies of IL-2 (turquoise), a potent cytokine- signaling protein—swing into action. Just as occurs during natural immune responses, IL-2 activates the T cells by binding to their IL-2 receptors (purple), causing the targeted T cells to proliferate and boosting their aggressiveness as they home in on and kill head-and-neck cancer cells.
By training, Einstein professor Steven Almo, Ph.D., is a structural biologist who uses X-ray crystallography to study the structure and function of molecules. His expertise has led to collaborations with researchers modifying proteins to create new therapies and with other researchers studying molecules that control the immune system. One day in 2010, those collaborations inspired what he calls “a crazy idea” for an experiment. “That will never work,” he recalls a colleague telling him. “You’re right,” agreed Dr. Almo. “But let’s try it anyway.”
The crazy idea was to mimic what the immune system does naturally when confronted with a potential danger such as a cancer cell: activate a select group of T cells to go on the attack.
Today’s immunotherapies—checkpoint-inhibitor drugs such as Keytruda and Opdivo—can cause serious side effects because they activate all the body’s T cells, triggering an overzealous immune response that extends to healthy organs and tissues. A targeted T-cell response would ideally kill cancer cells without endangering the patient. But creating a molecule to switch on specific T cells is complicated, says Dr. Almo. “I suspect that others had the same idea but talked themselves out of it, assuming it would be too challenging to make such a molecule.”
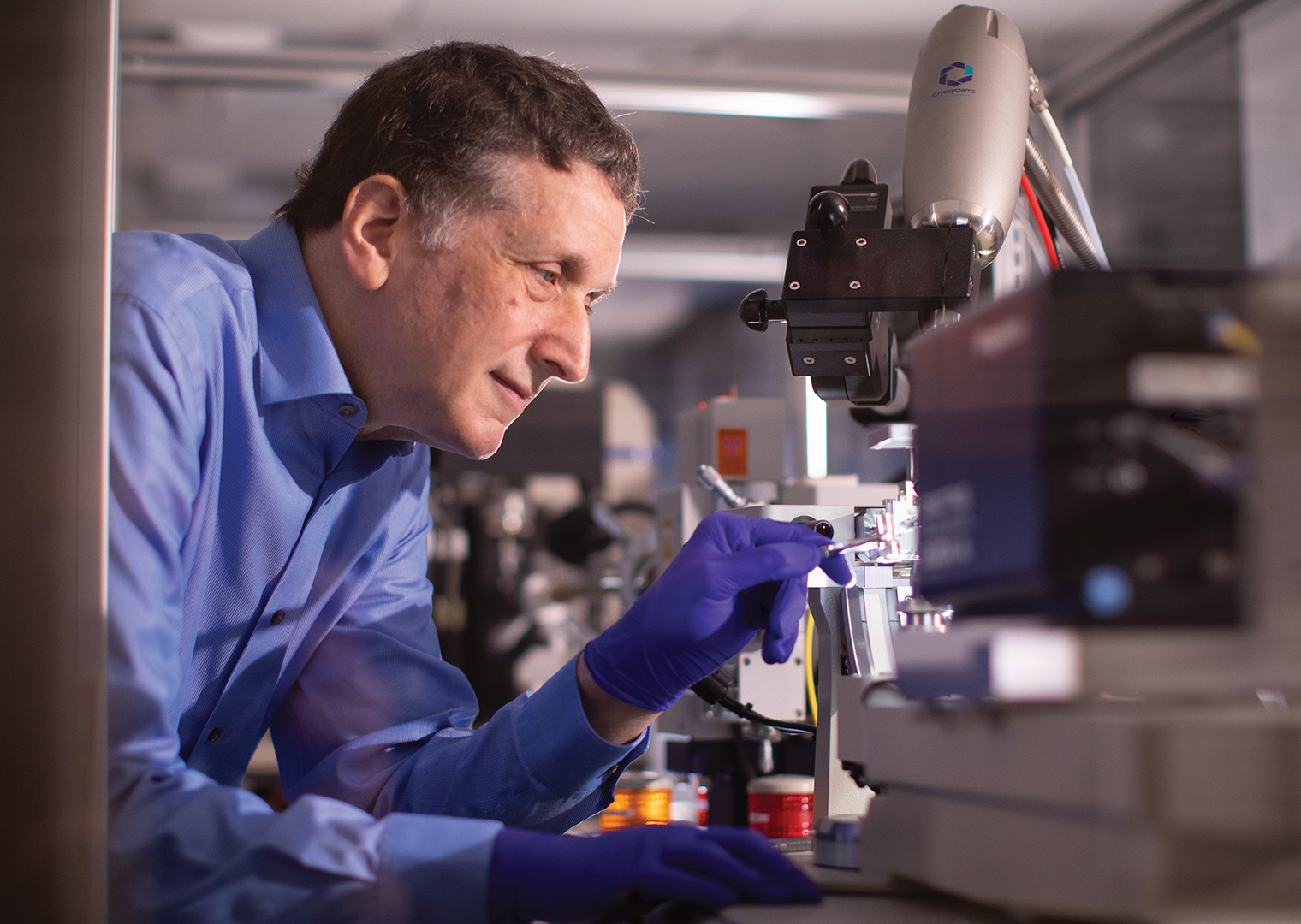 Steven Almo, Ph.D., develops drugs to selectively turn T cells on. (Photo by Jason Torres)
Steven Almo, Ph.D., develops drugs to selectively turn T cells on. (Photo by Jason Torres)
Dr. Almo’s idea was to synthesize fusion proteins equipped with two pairs of arms; one pair would bind only to those T cells pertinent to a patient’s disease, while the other would tell the disease-related T cells what to do. (See illustration above.)
That strategy could potentially treat many diseases in which T cells play a role. For treating prostate cancer, for example, the fusion protein would be tailored to seek out prostate-cancer-relevant T cells and then, with its second pair of arms, stimulate those T cells to replicate and infiltrate the tumor; for an autoimmune disease such as lupus, the fusion protein’s second pair of arms would be programmed to suppress, rather than stimulate, T-cell activity that would injure the body.
“To our surprise and delight we were able to make these fusion proteins and demonstrate in a test tube that they could kill specific T cells or make other T cells proliferate,” says Dr. Almo. “Those were the basic studies that led to the founding of the biopharmaceutical company Cue Biopharma and its licensing of our discovery from Einstein, which eventually led to clinical trials.”
Cue Biopharma, Inc., has advanced Dr. Almo’s technology, known as Immuno-STAT, through animal studies to clinical trials. In a two-arm, phase 1 multicenter trial that began in 2019, Cue Biopharma is evaluating an Immuno-STAT drug product named CUE-101 in patients with recurrent, metastatic head and neck squamous-cell carcinoma caused by human papilloma virus (HPV) 16. In the first part of the study, patients are treated with CUE-101 alone; in the second arm, patients receive CUE-101 together with the checkpoint inhibitor Keytruda.
A phase 2 study of CUE-101, underway at the Washington University School of Medicine, involves patients with newly diagnosed, locally advanced oropharyngeal squamous-cell carcinoma caused by HPV 16. Patients are receiving CUE-101 as neoadjuvant therapy (treatment intended to shrink tumors) one month before undergoing surgery for tumor removal.
“This study is especially important,” says Dr. Almo, “because examining the excised tumors allows you to actually see how CUE-101 has affected them.”
A tweak to CUE-101 has created a second Immuno-STAT drug, CUE-102. It’s designed to treat cancers in which the protein Wilms’ tumor 1 is overexpressed—a common occurrence in solid tumors such as breast, lung, colorectal, and pancreatic cancer and in blood cancers such as acute myeloid leukemia.
Since the FDA found that CUE-101 has a “favorable tolerability profile,” the agency has allowed a phase 1 trial of CUE-102 to begin at a much higher initial dose. “This significantly speeds up clinical development,” says Dr. Almo, saving nearly a year on studies that would otherwise be needed to find the highest safe dose.
“What’s most exciting to me,” he adds, “is that Montefiore Einstein is one of the sites where the CUE-102 clinical trial will be conducted.”