Many infectious-disease experts contend that it’s not a matter of if but when another pandemic will arise. Sooner or later, some combination of climate change, urbanization, international travel, human migration, drug resistance, and gene mutation will conspire to transform a run-of-the-mill pathogen into a highly contagious agent, capable of quickly spreading beyond its usual hosts and habitats and causing worldwide havoc.
“We were lucky with SARS-CoV-2 [the virus that causes COVID-19],” says Kartik Chandran, Ph.D., professor of microbiology & immunology, the Gertrude and David Feinson Chair in Medicine, and the Harold and Muriel Block Faculty Scholar in Virology at Einstein. “We greatly benefited from preexisting research on SARS-CoV, a closely related coronavirus. And we rapidly adapted newly available protein-engineering strategies and mRNA-expression technology to make highly effective vaccines against SARS-CoV-2. But there was no guarantee that all this and more would fall into place. We may not be so lucky the next time around.”
Einstein scientists are working to make the United States and the world better prepared for the next pandemic—whether it’s caused by newer microbes such as Crimean-Congo hemorrhagic fever or age-old killers such as the malaria parasite.
As of December 2023, the coronavirus SARS-CoV-2 had caused more than 772 million cases of COVID-19, including nearly 7 million deaths. Is there another deadly coronavirus in our future, or will an entirely different microbe spawn the next pandemic?
“There are many groups of viruses that concern me,” says Dr. Chandran. “We can make educated guesses about future outbreaks, but that’s all. Strange and unpredictable things happen in the world of infectious diseases.”
Echoes of Dr. Chandran’s answer appear in the National Institute of Allergy and Infectious Diseases’s 2021 Pandemic Preparedness Plan, a sweeping federal program designed to address the uncertainties inherent in safeguarding global health from communicable diseases. The two-part plan focuses on “priority pathogens” and “prototype pathogens”—basically, the knowns and unknowns of the viral world.
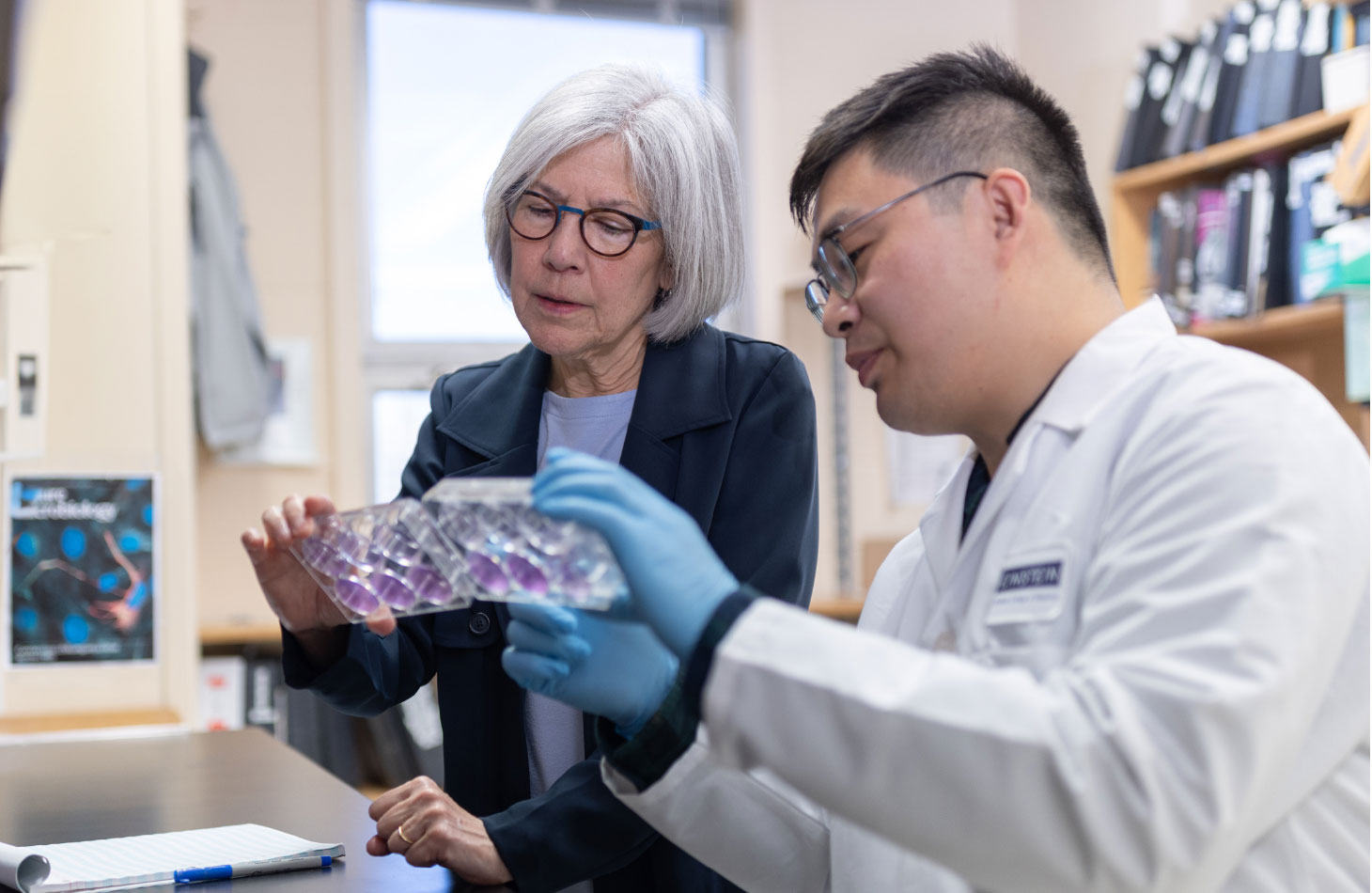
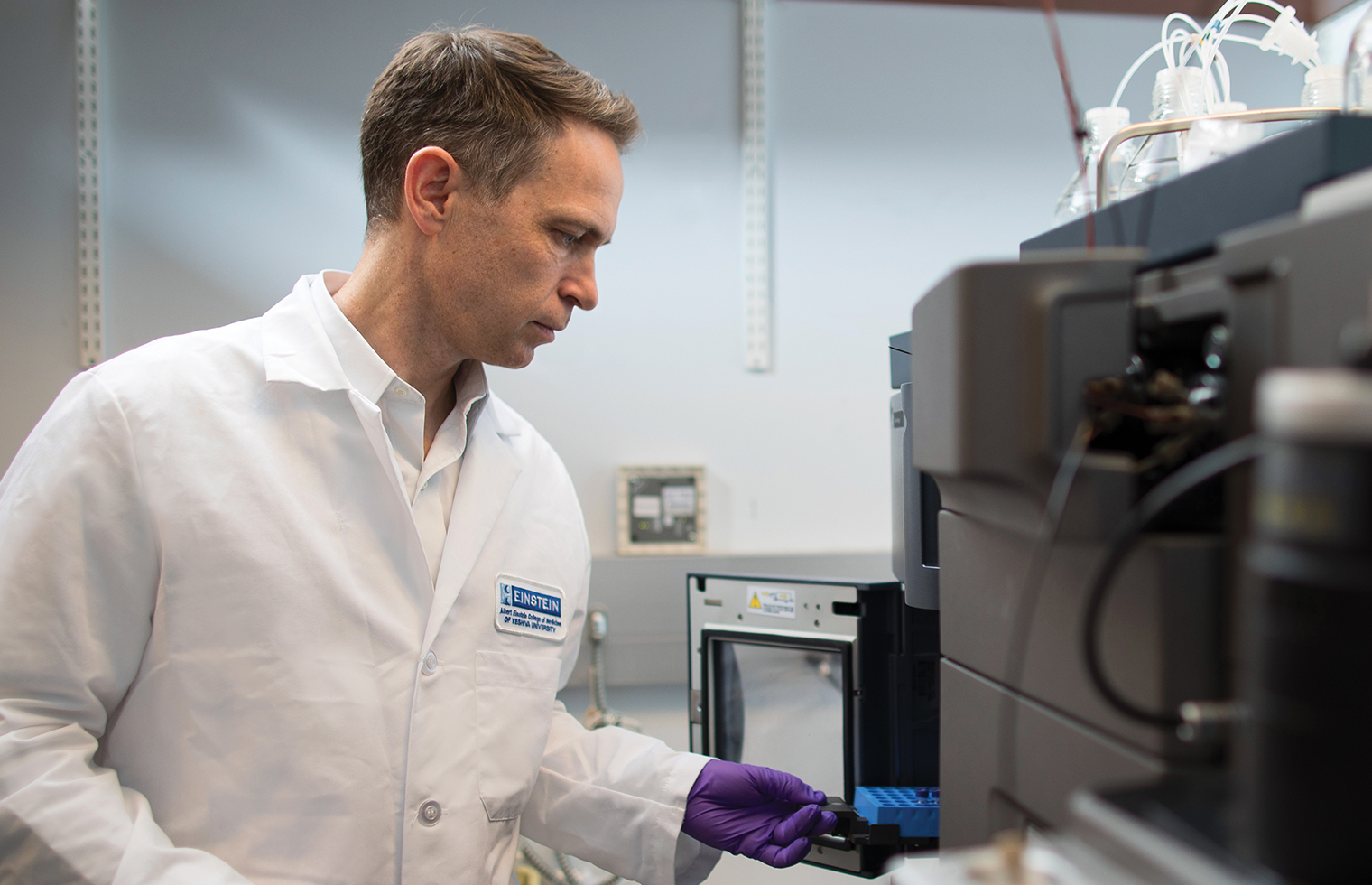
 Kartik Chandran, Ph.D., right, is working to develop blueprints for “plug-and-play” vaccines and antibody therapies to counteract emerging viruses.
Kartik Chandran, Ph.D., right, is working to develop blueprints for “plug-and-play” vaccines and antibody therapies to counteract emerging viruses.
Priority pathogens include viruses that scientists already know can cause significant human illness or death, such as dengue virus and Zika virus.
Prototype pathogens include viruses in families that have the potential to cause significant human disease. The idea here is to select representative viruses from each family, study them, and then develop countermeasures that will work against all viruses within that family. In keeping with the prototype-pathogen approach, Dr. Chandran is co-leading an unprecedented, multi-institutional effort to get ahead of the next pandemic.
That effort, called PROVIDENT (Prepositioning Optimized Strategies for Vaccines and Immunotherapeutics Against Diverse Emerging Infectious Threats), will develop blueprints for “plug-and-play” vaccines and antibody therapies to counteract emerging viruses belonging to three families: nairoviruses, transmitted by ticks (e.g., Crimean-Congo hemorrhagic fever), hantaviruses, spread by rodents (e.g., hantavirus pulmonary syndrome), and paramyxoviruses, spread by humans (e.g., mumps and measles).
“This kind of approach allowed us to move quickly during the COVID-19 pandemic,” says Dr. Chandran. “What we had learned from previous coronavirus-caused episodes—SARS [severe acute respiratory syndrome] in 2002 and MERS [Middle Eastern respiratory syndrome] a decade later—helped us create diagnostics, therapeutics, and vaccines against SARS-CoV-2.”
What we had learned from previous coronavirus-caused episodes—SARS in 2002 and MERS a decade later—helped us create diagnostics, therapeutics, and vaccines against SARS-CoV-2.
— Dr. Kartik Chandran
All told, PROVIDENT will link 13 teams in academia, government, and industry that will conduct four projects:
If and when a pathogen threatens to follow in SARS-CoV-2’s footsteps, Dr. Chandran and his PROVIDENT colleagues will be ready to respond rapidly to prevent or at least slow the next pandemic.
“PROVIDENT’s goal is more than just creating a therapy or vaccine for whatever future pandemic emerges,” Dr. Chandran says. “It’s designed to include the expertise capable of discovering new therapeutics and commercializing them—to get shots in arms, so to speak, at the earliest possible time to save as many lives as possible.”

Jonathan Lai, Ph.D., the Dan Danciger Professor of Biochemistry at Einstein, doesn’t have a crystal ball for predicting future pandemics, but many viruses give him pause. He’s worried about surges of West Nile, Zika, and eastern equine encephalitis in the United States and dengue, chikungunya, and Ebola overseas. In all those cases, humans have little or no defense—natural or pharmaceutical—against the microbes responsible.
SARS-CoV-2, the respiratory virus that caused the COVID-19 pandemic, isn’t on his list, largely because of widespread herd immunity and effective vaccines.
With Powassan, a tick doesn’t have to engorge blood and can transmit the virus in just 15 minutes.
— Dr. Jonathan Lai
“I’m more concerned about unknown viruses that are almost certainly lurking somewhere in a bat cave in the wilderness,” says Dr. Lai, who also collaborates with Dr. Chandran on PROVIDENT. “As urbanization continues to push people farther and farther into the forest, we’re increasing our exposure to viruses found in animals. All it takes is a single adaptive mutation for one of those viruses to find a new host—perhaps in one of us.”
Dr. Lai also worries about a familiar, but ever-changing, respiratory virus: influenza, which kills an estimated 400,000 people each year. “The global burden of seasonal flu is greatly underappreciated,” he says. “There are a lot of coronavirus variants, but influenza viruses are even more diverse with respect to their antigens. This diversity makes it challenging to come up with a new vaccine each year, and those vaccines usually are not very effective.”
 Jonathan Lai, Ph.D., at left, focuses on developing novel immunotherapies and vaccine candidates for a wide range of pathogens.
Jonathan Lai, Ph.D., at left, focuses on developing novel immunotherapies and vaccine candidates for a wide range of pathogens.
Over the years, Dr. Lai has focused on developing novel immunotherapies and vaccine candidates for a wide range of pathogens, including Ebola, chikungunya, SARS-CoV-2, and dengue. He has recently added a new emerging pathogen to his list: Powassan virus, named after the town of Powassan, Ontario. Powassan virus was first identified there in 1958, when it was isolated from the brain of a young boy who had died from the infection.
Powassan virus disease causes severe brain inflammation when the virus invades the central nervous system; 10% to 15% of those cases are fatal, and half the survivors have long-lasting neurologic deficits such as headaches and cognitive problems.
Powassan virus is primarily transmitted by the bites of deer ticks—the same tick species that carries Lyme bacteria. There are no approved vaccines or therapies.
Lyme disease has shown that tick-borne pathogens such as Powassan virus should not be underestimated. Today, just a few decades after it first appeared, Lyme is responsible for a half-million infections a year in the United States, many of which linger for months or years. Powassan has the potential to spread even faster.
“In order to infect you with Lyme bacteria, a tick has to bite you and then engorge itself with your blood, which can take hours,” says Dr. Lai. “With Powassan, a tick doesn’t have to engorge blood and can transmit the virus in just 15 minutes.”
The ability of the nanoparticle to elicit protective antibodies in these mice shows that it also has potential for use as a vaccine for preventing Powassan virus disease.
— Dr. Jonathan Lai
Powassan virus disease is not especially common, but cases are on the rise—and Dr. Lai suspects that more infections are occurring than are being reported. He and Emily Miller, M.D., Ph.D., assistant professor of medicine and of microbiology & immunology at Einstein, are now collaborating with the U.S. Military Academy at West Point to determine the prevalence of infections among Army cadets, a particularly vulnerable population. “They’re the ones out in the fields, and that’s where the ticks are,” he says.
In a 2022 paper in PLOS Pathogens describing their Powassan virus research, Dr. Lai and colleagues reported findings that could lead to a monoclonal antibody therapy as well as a vaccine.
The researchers immunized mice with nanoparticles bearing EDIII, a part of Powassan virus’s glycoprotein envelope. When serum from immunized mice was transferred to uninfected mice, it protected them from a dose of Powassan virus that would ordinarily prove fatal. The researchers then isolated the monoclonal antibodies responsible for this protection and found four of them that showed especially potent antiviral activity.
“The ability of the EDIII nanoparticle to elicit protective antibodies in these mice shows that it also has potential for use as a vaccine for preventing Powassan virus disease,” Dr. Lai says. “As Powassan virus becomes more widespread and thus a pathogen of increasing concern, we hope to be prepared with monoclonal antibody therapies and a vaccine to combat it.”


Chikungunya virus, another mosquito-borne pathogen, doesn’t cause nearly so many infections as the malaria parasite. But it’s significant enough to be classified as an “emerging global health threat” by the U.S. Food and Drug Administration (FDA).
Health officials now report about a half-million cases of chikungunya each year, mostly in Central and South America, with smaller outbreaks in Asia and Africa. And climate change is gradually expanding the territory of the mosquitoes (Aedes aegypti and Aedes albopictus) that transmit the virus. No antiviral treatments for chikungunya are available yet, although deaths from the infection are relatively rare.
“It’s probably just a matter of time until the disease becomes more widespread,” says Einstein’s resident chikungunya expert, Margaret Kielian, Ph.D., professor of cell biology and the Samuel H. Golding Chair in Microbiology.
In a glimmer of good news, the FDA recently approved the world’s first vaccine to protect against chikungunya virus infection. Yet the single-shot vaccine’s high cost (currently $350) means it will be little used in the countries where it’s most needed. And with growing vaccine hesitancy in the United States and around the world, the availability of an effective form of prevention is no guarantee against widespread outbreaks or even a pandemic.
Three to seven days after being bitten by an infected mosquito, people may have symptoms of fever and intense joint pain—a fact reflected in chikungunya’s name, which means “bent over in pain” in Makonde, an African language.
While symptoms usually improve within a week, some 20% to 30% of patients experience chronic and debilitating arthritis—suggesting that some copies of the virus are able to avoid the body’s immune response. How the virus is able to persist in these patients has long been a mystery.
 Margaret Kielian, Ph.D., and postdoctoral fellow Peiqi Yin, Ph.D., discovered a mode of chikungunya virus transmission that could explain why symptoms of the infection persist for months or years.
Margaret Kielian, Ph.D., and postdoctoral fellow Peiqi Yin, Ph.D., discovered a mode of chikungunya virus transmission that could explain why symptoms of the infection persist for months or years.
If we can generate the production of such antibodies in human patients, that could help combat the chronic symptoms of chikungunya infection.
— Dr. Margaret Kielian
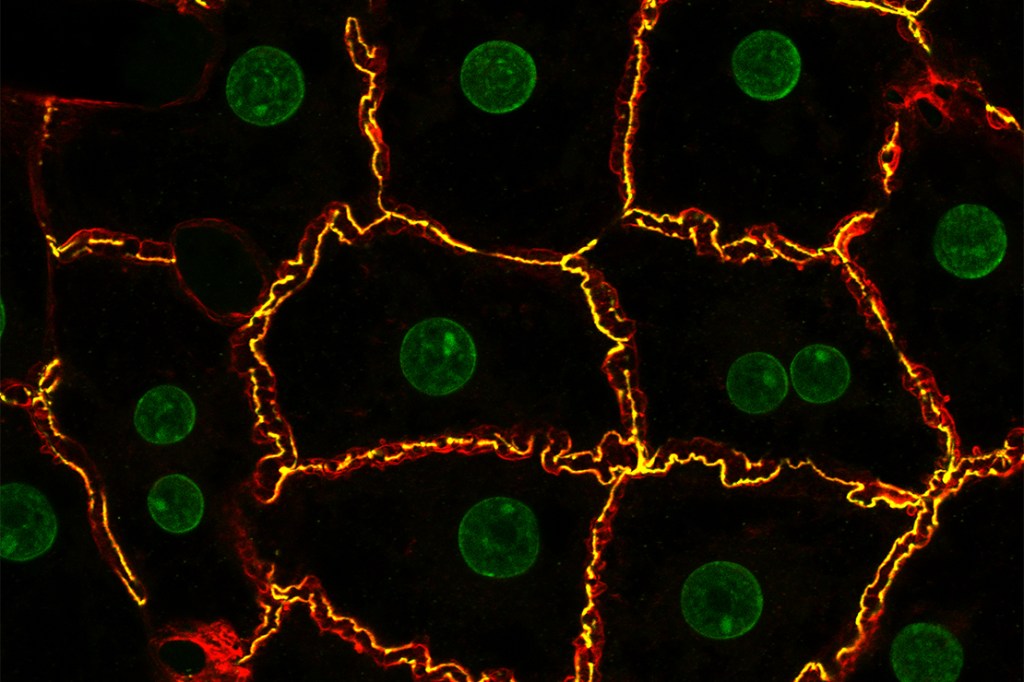
Chikungunya virus was thought to spread in the body by infecting a cell, replicating within that cell, and then sending copies of itself into the bloodstream to infect new cells.
“However, we’ve found that the virus can also spread by hijacking a host cell’s cytoskeleton—the proteins that support cells and maintain their shape,” Dr. Kielian says. “The virus causes the infected cell to send out long, thin extensions that make stable contacts with uninfected neighboring cells, enabling the virus to safely and efficiently travel from one cell to another.” She and her colleagues call these virus-induced structures “intercellular long extensions,” or ILEs.
“This mode of viral transmission may not only shield some copies of the virus from the host’s immune response but could also explain why symptoms of chikungunya infection can persist for many months or years,” adds Peiqi Yin, Ph.D., a postdoctoral fellow in Dr. Kielian’s lab.
The researchers also found that certain antiviral antibodies were able to block ILEs from forming and prevent cell-to-cell transmission. “If we can generate the production of such antibodies in human patients, or develop other methods to stop ILE formation, that could be especially helpful in combating the chronic symptoms of chikungunya infection,” says Dr. Kielian, whose findings were published in Nature Microbiology in 2023. Her research might also lead to an improved vaccine.
“We’re currently mapping the precise sites on the virus to which those blocking antibodies bind,” Dr. Kielian says. “We’ve also found that sera from convalescent patients can block ILEs from forming. This suggests that it might be possible to develop a vaccine that works by generating ILE-blocking antibodies.”


Now that COVID-19 has receded somewhat into the background, an ancient disease is positioned to reclaim its long-standing title as the world’s most deadly infectious disease: tuberculosis (TB), caused by inhaling Mycobacterium tuberculosis (Mtb) bacteria.
“From a global perspective, I would argue that the next pandemic is already here,” says Michael Berney, Ph.D., associate professor of microbiology & immunology at Einstein. “It’s just slipped our minds because TB is not so prevalent in this part of the world.”
In 2022, the United States reported just 8,000 cases of TB, resulting in 600 deaths. During that same year, more than 10 million cases and 1.3 million fatalities from this respiratory disease occurred worldwide, even though it is preventable and curable. Recent advances in diagnosing and treating TB have begun to reach the hardest-hit countries. Resources are not sufficient to help everyone in need, however, and so the TB pandemic continues.
According to the World Health Organization, 40% of people with TB haven’t been diagnosed and therefore aren’t being treated. Without therapy, someone with TB will spread the disease to an average of 15 people per year. Dr. Berney is particularly worried about the rise of multidrug-resistant or extensively drug-resistant TB, which already accounts for 3% to 4% of all cases, causing around 15% of all TB deaths.
“We are not well prepared for a significant rise in drug resistance, neither in resource-limited settings nor in high-income countries, including the United States,” notes the researcher. Such infections are highly lethal, forcing clinicians to use second-line drugs that often cause more-severe side effects than first-line drugs.
 Michael Berney, Ph.D., works on tuberculosis drug development.
Michael Berney, Ph.D., works on tuberculosis drug development.
“One reason for drug-resistant Mtb is that standard first-line drugs have to be taken for at least four months, and cause nasty side effects,” says Dr. Berney. “As a result, patients often don’t comply with the regimen—and their reduced drug intake allows drug-resistant strains to arise. Unfortunately, the second-line drugs needed for drug-resistant cases cause even more-severe side effects, and poor adherence that can lead to even more drug-resistant strains.”
Mtb’s increasing drug resistance urgently requires a new generation of anti-TB drugs. “But unfortunately,” says Dr. Berney, “many pharmaceutical companies have reduced or stopped investing in TB research. They assumed that the latest generation of TB medications would be sufficient and, frankly, they have little financial incentive to continue this work. That’s why we in academia are compelled to study neglected diseases like TB, to identify promising new compounds that companies can license and develop into drugs.”
For his part, Dr. Berney is bolstering basic research and drug development. One of his projects, funded by the National Institutes of Health (NIH), focuses on a lipid found in the outermost layer of Mtb bacteria. The lipid, known as PDIM, forms a protective barrier that wards off both TB drugs and the host immune system and greatly enhances virulence. His findings were published in May in Nature Microbiology.
We are not well prepared for a significant rise in drug resistance, neither in resource-limited settings nor in high-income countries, including the United States.
— Dr. Michael Berney
“Those lipids are usually lost when you culture Mtb in the lab—a problem that has confounded TB studies for 50 years,” he explains. “Without these lipids, Mtb is much less virulent, and the cell membrane becomes more permeable, making it appear that some anti-TB drugs you’re evaluating are more effective than they actually are.”
Dr. Berney’s group recently discovered that this loss of PDIM is caused by a metabolic deficiency that occurs when Mtb is grown in culture media—a problem that can be remedied by adding odd-chain fatty acids, cholesterol, or vitamin B12.
His team also developed a simple and efficient test for checking whether lab-grown Mtb is producing PDIM. Its findings greatly improve experimental precision and reproducibility in TB research—for example, in drug discovery, vaccine development, and host-pathogen interactions. TB researchers worldwide stand to benefit from these findings.
A second innovation from the Berney lab also promises to speed up drug discovery. Most screening tests for potential TB drugs show only whether a compound inhibits the bacterium in culture, meaning that time-consuming and costly follow-up tests are still needed. That may soon change. Dr. Berney and his colleagues at the University of Basel (a public research university in Switzerland) have devised a new assay for assessing whether, and how, a given compound affects Mtb’s metabolism—a good indicator of its mechanism of action and therapeutic potential.
Under a grant from the NIH, Dr. Berney is using the new assay to evaluate more than 500 compounds that were shown to inhibit Mtb in culture but were shelved for lack of time and resources for additional investigation.
“With our screening tool, we can quickly determine a compound’s metabolic fingerprint and, importantly, whether the compound targets TB bacteria in a novel way. Then we can make better-informed decisions about compounds that merit further evaluation,” Dr. Berney says.




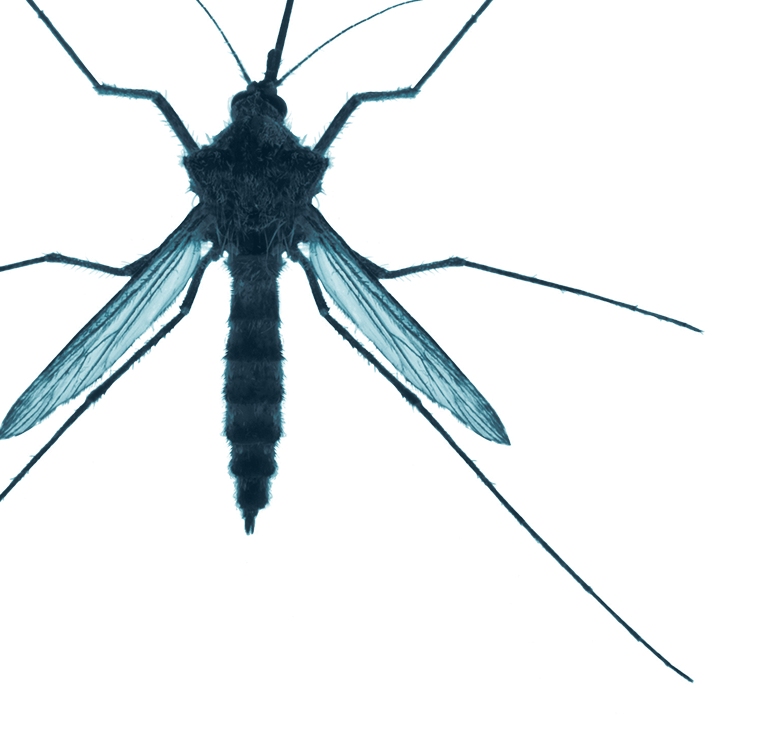
Malaria is another ancient disease that continues to plague humankind. Almost 250 million cases of malaria occur each year, resulting in hundreds of thousands of deaths and untold suffering, mostly in sub-Saharan Africa but also in parts of Latin America and South Asia. Consistent use of antimalarial medications, plus mosquito-control measures such as bed nets, window screens, and insecticides, keeps malaria in check in some areas, but that’s the exception, not the norm.
Anopheles mosquitoes, which carry malaria-causing Plasmodium parasites, are already in many parts of the world, including southern areas of Europe and the United States. As the globe warms, those mosquitoes are likely to enter new regions. Last year, for example, nine locally transmitted cases of malaria were reported on U.S. soil—the first such cases in two decades, and perhaps a sign of things to come. But that’s not what keeps an Einstein malaria expert up at night.
Malaria is already a global infection, with half the world’s population now at risk.
— Dr. Johanna P. Daily
“Malaria is already a global infection, with half the world’s population now at risk,” says Johanna P. Daily, M.D., M.S., professor of medicine and of microbiology & immunology at Einstein and an infectious-disease physician at Montefiore. “The bigger issue is ‘How do we decrease its transmission in rural Africa, where most of the morbidity and mortality is occurring?’”
Dr. Daily is especially concerned about malaria’s impact on children. In Africa, children under 5 account for about 80% of all malaria deaths; many of those deaths are due to cerebral malaria, which is primarily seen in children and leads to severe brain swelling and coma. Cerebral malaria is not invariably fatal; most patients respond to antimalarials and regain consciousness in a couple of days, although a substantial number suffer long-term cognitive deficits.
“The true burden of cerebral malaria and its long-term effects on these children is hidden,” Dr. Daily says. “Here in the United States, we could test for and treat cerebral malaria and provide rehabilitation in the case of neurological damage. But in Africa they just don’t have the tools for diagnosing cerebral malaria or treating its neurological consequences.”
Until now, little has been known about why cerebral malaria strikes some children but not others. Dr. Daily and her colleagues in Malawi, Africa, may recently have found the reason.
 Johanna Daily, M.D., M.S., studies the burden of cerebral malaria and its long-term effects on children.
Johanna Daily, M.D., M.S., studies the burden of cerebral malaria and its long-term effects on children.
“We compared the blood of children with cerebral malaria in full coma with the blood of kids who had mild infections but were healthy enough to be running around and playing. The only significant difference was that the kids with cerebral malaria had abnormally high concentrations of pipecolic acid [an amino acid] in their blood,” she says.
Dr. Daily discovered decades-old studies linking pipecolic acid with neurological abnormalities, but it had never been associated with cerebral malaria. What might it be doing in these young patients?
Using a mouse model of cerebral malaria, Dr. Daily found that when the blood-brain barrier becomes increasingly permeable—as occurs during severe malaria—very high levels of pipecolic acid accumulate in the brain. Her findings were published in 2022 in the Journal of Infectious Diseases.
Work in her lab and other labs suggests that pipecolic acid is produced by the malaria parasite itself. And since children with cerebral malaria have a larger parasite burden than children with run-of-the-mill malaria, that would explain their higher pipecolic-acid levels and neurological complications. Children with cerebral malaria also tend to have compromised kidney function, making them less able to clear excess pipecolic acid from the bloodstream.
Under a grant from the NIH, Dr. Daily is investigating how the parasite produces pipecolic acid. The research will also test her hypothesis—suggested by previous animal studies—that pipecolic acid causes unconsciousness by stimulating GABA receptors (a class of receptors that respond to the neurotransmitter gamma-aminobutyric acid, or GABA).
Ideally, this work will solve a longtime mystery: why cerebral malaria causes coma. Clinically, the research may lead to rapid and inexpensive tests for predicting which children with malaria parasites are likely to develop cerebral malaria; it may also identify novel drug targets for improving the health of children with this potentially fatal form of the disease.