Error: No layouts found
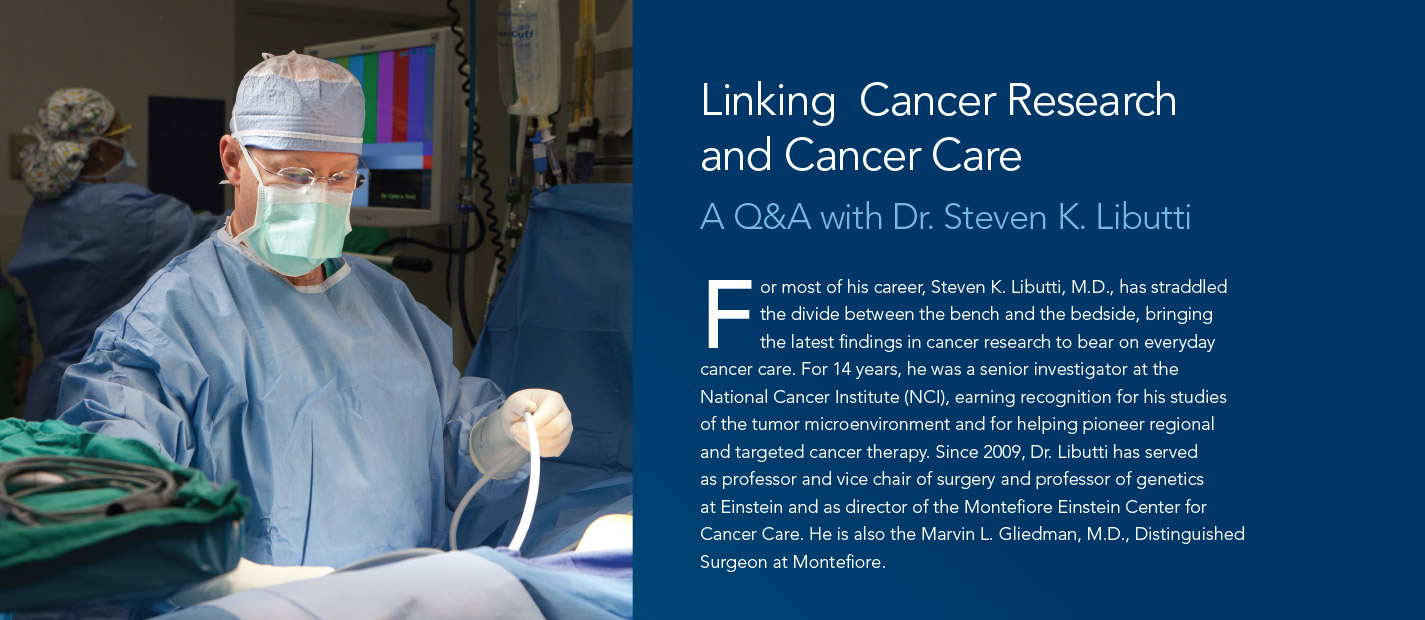
I was very interested in sports, and my initial goal was to do orthopedics and sports medicine. That led me to surgery and then to cardiac surgery, because of the world-class surgeons at Columbia, including Robert Michler [now chair of surgery at Einstein and Montefiore]. In the middle of my residency, I had an epiphany that while cardiac surgery was amazing, I also had a passion for research, and I wasn’t compelled by the questions needing to be answered in cardiology. Eventually, I realized that oncology was the best match for my skills as a surgeon and a researcher.
My grandmother was diagnosed with pancreatic cancer when I was a freshman in college. She went from this vibrant woman to a frail skeleton of a person within six months. Seeing how someone could deteriorate so quickly had a tremendous impact on me.
That can be summed up by a quote from the 18th-century surgeon John Hunter: “Surgery is like an armed savage who attempts to get back by force what a civilized man would get by stratagem.” Surgery, with few exceptions—and particularly for solid tumors—is the only modality we have that can cure cancer, although that may soon change with immunotherapy. But while surgery is a powerful tool, it is also traumatic for the patient. Anyone who thinks that we can fix all cancers mechanically is being arrogant and simplistic. We need other strategies.
It really hasn’t been a war but rather a very long thesis on the disease. Slowly, we’ve been learning about the pathways that lead to cancer and how to manipulate those pathways to eradicate, or at least control, the disease. We’ve made progress against the most common cancers—colon, lung, breast and prostate—and overall, there are fewer deaths due to cancer now than there were 15 years ago.
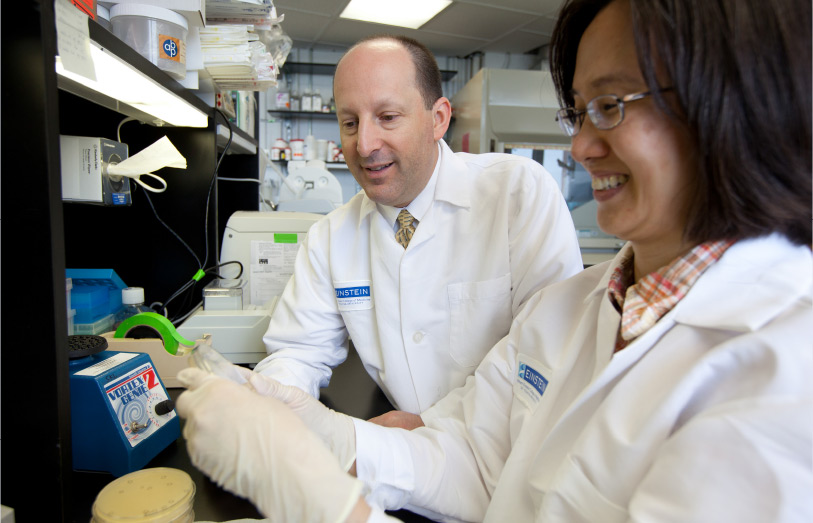
The NCI’s intramural research program is a wonderful place, where your patients are a hallway away from your laboratory. It’s ideal for taking ideas from the clinic to the lab and back again in the form of new therapies. But the program is relatively small. After 14 years, I began to realize that to have a bigger impact, I needed to be on a different stage, such as an academic medical center. With perfect timing, Steven Safyer [president and CEO of Montefiore Medicine] and Allen Spiegel [dean of Einstein] offered me an exciting opportunity to help lead the effort to bridge cancer research at Einstein with the clinical capabilities at Montefiore.
One is the collaboration between John Condeelis, an Einstein basic scientist, and Joseph Sparano, a clinical researcher in oncology at Einstein and Montefiore. Dr. Condeelis studies the factors in the tumor microenvironment that promote the spread of breast cancer. Dr. Sparano brings in-depth knowledge of agents that might be able to target those mechanisms, plus extensive experience in carrying out clinical trials to evaluate therapies for breast cancer and other malignancies.
Another example is my work with Lakshmi Rajdev, a medical oncologist at Einstein and Montefiore. Dr. Rajdev asked me if we could treat neuroendocrine tumors more effectively by taking advantage of the discovery that the mTOR pathway plays an important role in these malignancies. Using a transgenic mouse model of neuroendocrine tumors—developed at the NCI and refined here—we tested an agent that can hit two different targets within the mTOR pathway. We’ve since shown that this treatment is more effective than single-agent therapy in this model, and we now have approval for an NCI-sponsored clinical trial.
Yes, several. For instance, we have a pilot study in which we’ll take T cells from a patient with a solid tumor and transform them in the lab. We’ll “infect” the T cells with a retrovirus carrying the gene for an artificial T-cell antigen receptor. This means that the gene is designed to express a receptor on T cells that recognizes and binds to an antigen on the patient’s tumor called NY-ESO-1. These engineered T cells will be expanded in number and then returned to patients, providing a personalized therapy for their cancer. NY-ESO-1 is expressed in about 30 percent of solid tumors, so this approach could have wide application. This modified T-cell antigen receptor was developed at the NCI. But we now have the infrastructure here at Einstein that will allow our talented scientists—such as Ulrich Steidl, Amit Verma and Chandan Guha—to identify new targets and develop new antigen receptors. This Einstein-Montefiore collaboration will allow us to ask and answer questions at the cutting edge of immunotherapy.
One change was to get away from the traditional cancer-care model—where a patient goes from one physician to the next—and instead have patients engage all their providers in a single program. This relieves patients, and maybe even their primary care doctors, of the burden of coordinating cancer care. We’ve also improved our ability to conduct clinical trials by expanding our patient population. In the years I’ve been here, Montefiore has grown from three hospitals in the Bronx into a health network encompassing 12 hospitals with various levels of affiliation in the Bronx and in Westchester, Rockland and Orange Counties.