Of all the heartbreaking events of my father’s long, slow demise from Alzheimer’s disease, the most devastating was when he turned to my mother and said, in a rare moment of clarity, “I can’t do this anymore.” My father was diagnosed with Alzheimer’s—the most common type of dementia, accounting for 60% to 80% of cases—in the late 1990s.
In hindsight, the first signs had appeared years earlier. Out of nowhere, he began insisting that the front door must always be locked. My parents lived in a quiet, upscale suburb of New York City. Such fear made no sense, especially coming from a proudly self-reliant man and veteran world traveler. I would learn later that heightened anxiety is a common harbinger of dementia.
Piece by piece, the things that defined my father began disappearing. He sold his business and retired. His confident New York City stride shortened to a halting shuffle. He faded into the background at family gatherings, a ghost of the patriarch we once knew. Depression darkened his days. “I was unable to read … or do things with my hands, which was very important to me,” my father said in a 2002 BBC Radio program on dementia research. “I used to do all kinds of artwork, photography, and carpentry.”
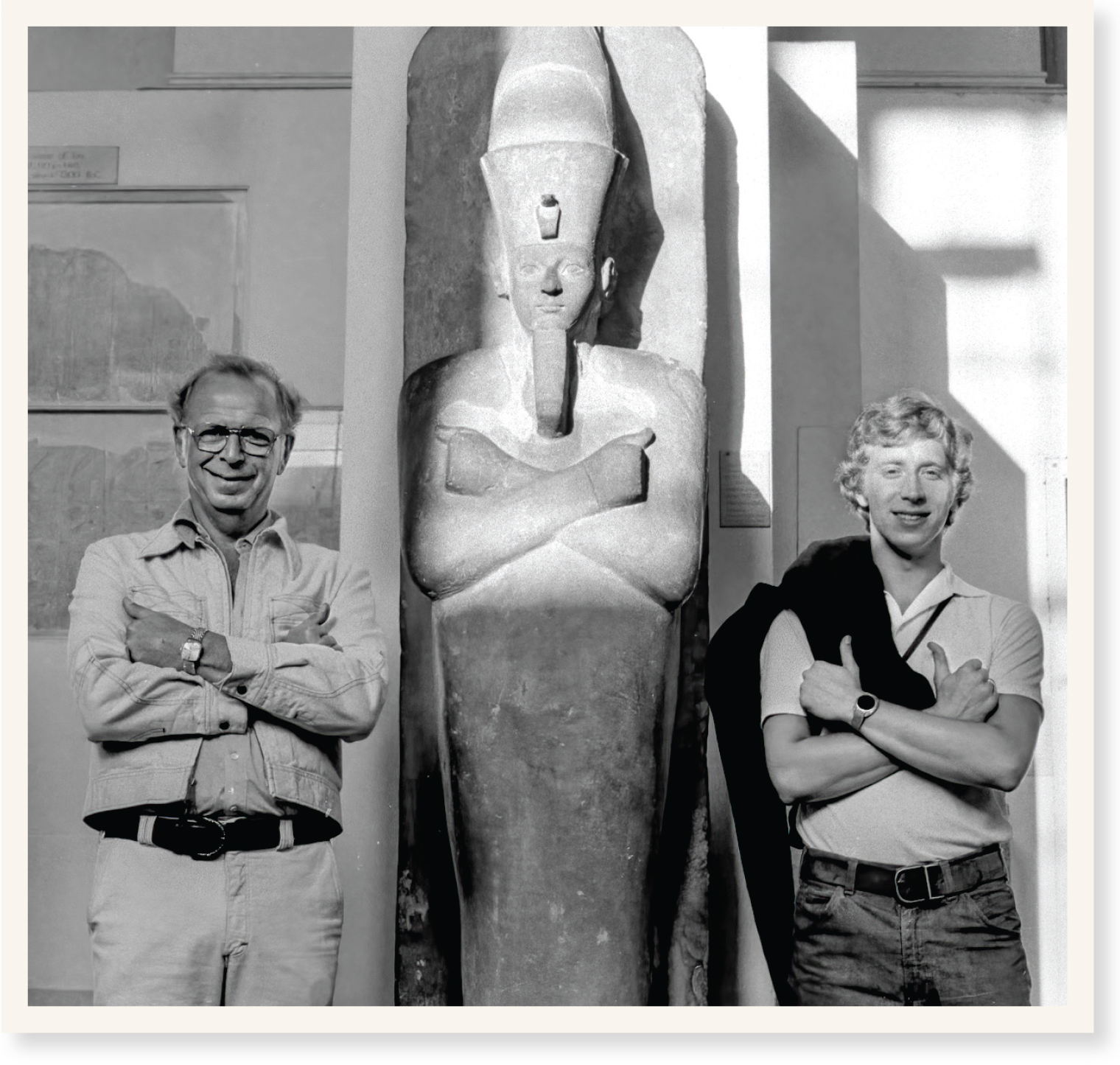 Author Gary Goldenberg with his father, Murray, at the British Museum in 1977.
Author Gary Goldenberg with his father, Murray, at the British Museum in 1977.
Early on, my father saw a neurologist at a Manhattan teaching hospital. She prescribed memantine and donepezil (the first two drugs approved to treat the disease) plus costly experimental infusions of immunoglobulins. They seemed to help—for a while.
“I was a vegetable before and I learned how to read again, write again,” my father told the BBC. But ultimately, nothing could stop the incoming tide of amyloid plaques and tau tangles from clogging his neurons, clouding his thoughts, and crippling his movements.
Millions of other American families have Alzheimer’s stories to tell, each unhappy in its own way. Fortunately, there is reason to hope that future stories may have happier endings.
I was unable to read or do things with my hands, which was very important to me. I used to do all kinds of artwork, photography, and carpentry.
—Mr. Goldenberg, the author’s father
Relatively little has changed in the world of Alzheimer’s care in the quarter-century since my father was diagnosed. Short of a brain autopsy, there is still no definitive diagnostic test for the disease, which robs people of the ability to remember new information and worsens over time.
The half-dozen drugs approved by the U.S. Food and Drug Administration (FDA) are only marginally effective. (Aduhelm, the most recent drug to win FDA approval, in 2021—and the first new Alzheimer’s drug in 18 years—may modestly decrease symptoms in people with mild cognitive impairment or early Alzheimer’s.)
On the positive side, basic researchers at Einstein are learning more about the molecular biology and genetics of the disease, moving tantalizingly close to new treatments. Clinical researchers at Einstein and Montefiore are improving early diagnosis, identifying risk factors that can be modified, and devising promising nonpharmacologic interventions for alleviating symptoms. And clinicians are fine-tuning dementia-care services, reducing patient distress, and easing the burden on family caregivers.

Perhaps the greatest Alzheimer’s mystery is why some people develop it and others don’t. Some combination of nature and nurture, genetics and environment, is clearly to blame, but trouble teasing apart the many contributing factors has hindered efforts to find treatments, much less cures.
Nir Barzilai, M.D., the Ingeborg and Ira Leon Rennert Chair in Aging Research, director of the Institute for Aging Research, professor of medicine and of genetics at Einstein, and an endocrinologist at Montefiore, has long posited that Alzheimer’s can best be understood by studying aging.
“Most chronic diseases arise from one primary cause, which is the biology of aging itself,” Dr. Barzilai notes in his book Age Later: Health Span, Life Span, and the New Science of Longevity (St. Martin’s Press, 2020). “While there are genetic and environmental bases for many age-related diseases, aging increases our chances of contracting them more than any other factor alone.”

While there are genetic and environmental bases for many age-related diseases, aging increases our chances of contracting them more than any other factor alone.
—Dr. Nir Barzilai
In 1998, Dr. Barzilai set out to reveal the secrets of people he calls SuperAgers—those rare individuals who continue to live independently at age 95 and beyond. That effort led to his Longevity Genes Project, funded by the National Institute on Aging (NIA), to identify genes that contribute to exceptional longevity in humans and learn how they stave off Alzheimer’s and other age-related diseases.
Over the past two decades, Dr. Barzilai’s research team has been studying more than 750 centenarians and near-centenarians, more than 1,000 of their offspring (ages 60 to 85), and about 900 age-matched unrelated participants (controls). The research has yielded important insights into successful aging.
You might assume that SuperAgers lead healthy lifestyles. Instead, says Dr. Barzilai, “many of them break the rules that the rest of us should be following. Nearly half the centenarians in our study are overweight or obese, nearly half smoke, and fewer than half do even moderate exercise. So something—most likely their genetic makeup—is slowing their aging enough so that their lifestyles don’t matter very much.”
For most people, genetics probably contribute just 20% to 25% to how well or badly they age, with the environment responsible for the rest. But the statistics are much different for centenarians: “Our studies suggest that centenarians’ genes are 75% to 80% responsible for how they age,” says Dr. Barzilai, “which is why we’re so intent on finding those genes and learning how certain of their variants contribute to longevity. By designing drugs that mimic the effects of those longevity-gene variants, we may be able to help prevent Alzheimer’s.”
Genes that appear to be implicated in aging and Alzheimer’s are involved in the insulin-like growth factor 1 (IGF-1) signaling pathway within cells. IGF-1 is a hormone that acts as insulin does in some tissues but whose primary job is to stimulate growth.
“Studies in many organisms, from fruit flies to worms to mice, have shown that the IGF-1 pathway regulates the rate of aging, longevity, and the risk for age-related diseases,” says Sofiya Milman, M.D., M.S., associate professor of medicine and of genetics and director of human longevity studies at the Institute for Aging Research at Einstein, and an endocrinologist at Montefiore. “The unanswered question was whether the highly conserved IGF-1 pathway is also relevant for human aging.”

Studies in many organisms, from fruit flies to worms to mice, have shown that the IGF-1 pathway regulates the rate of aging, longevity, and the risk for age-related diseases.
—Dr. Sofiya Milman
In research published in 2014 in Aging Cell, Dr. Milman found that female SuperAgers with lower IGF-1 levels lived significantly longer than female SuperAgers with higher levels; no survival advantage was seen in males. Next, in a 2016 paper in Aging, she analyzed IGF-1’s association with the cognition of SuperAgers. Just 22% of female SuperAgers with low IGF-1 levels showed signs of cognitive impairment, while 42% of those with high IGF-1 levels showed signs of impaired cognition. (For men, no significant association between IGF-1 levels and cognitive ability was found, perhaps because so few men were enrolled in the study.)
The benefits of low IGF-1 levels may also extend to the general population, not just centenarians. In a 2020 study of seniors (average age 76), Dr. Milman found evidence that low IGF-1 levels may be good for older people in general: Over a 10-year period, seniors with lower IGF-1 levels at enrollment had lower death rates, lower rates of chronic illnesses, and better cognitive function than those with higher levels. Other studies, however, have found that high levels of the hormone help prevent various diseases.
How can IGF-1 both help and harm? Dr. Milman suspected “antagonistic pleiotropy.” This theory of the evolutionary origin of aging, proposed in 1957, posits that certain genes that are beneficial in youth cause harm in old age. To see if this holds true for IGF-1, Dr. Milman analyzed clinical data from a study involving a half-million residents of the United Kingdom, ranging in age from 37 to 73. IGF-1 levels were measured at the start of the study, and participants were then followed for a decade. The results suggested that IGF-1 is indeed exerting antagonistic pleiotropic effects.
For both younger and older adults, a low serum IGF-1 level at the start of the study correlated with an increased risk of dying, especially in younger adults. Similarly, a high IGF-1 was associated with a higher mortality risk for both age groups—but the risk of dying (and especially of developing diabetes and vascular disease) was greater for older adults. The findings, as seen in the graph above, suggest that higher serum IGF-1 levels may be beneficial in youth but harmful at older ages.
Those findings should serve as a warning to seniors taking human growth hormone (HGH)—which triggers the production of IGF-1—to make themselves look and feel younger. “For them, the risks of using HGH as an antiaging strategy outweigh the potential benefits,” emphasizes Dr. Milman, whose paper on antagonistic pleiotropy was published in Aging Cell in 2021.
How might low levels of IGF-1 delay aging and promote cognitive resilience? Dr. Milman is seeking the answer in her latest study, supported by a $4 million grant from the NIA. “We’re looking specifically at how IGF-1 may impair autophagy, a natural cellular housekeeping process,” she says. “Autophagy is known to decline in most tissues with aging, and has been implicated in neurodegenerative diseases, including Alzheimer’s.”
The relationship of autophagy and Alzheimer’s is a focus of research by Ana Maria Cuervo, M.D., Ph.D., the Robert and Renée Belfer Chair for the Study of Neurodegenerative Diseases and a professor of developmental and molecular biology and of medicine and co-director of the Institute for Aging Research at Einstein.
Early in her career, Dr. Cuervo discovered one type of autophagy, dubbed chaperone-mediated autophagy (CMA). This selective recycling process involves specialized “chaperone” molecules that guide proteins to enzyme-filled organelles called lysosomes for destruction and recycling within the cell.
Our drug revitalizes CMA efficiency by boosting levels of a key CMA component.
—Dr. Ana Maria Cuervo
“CMA makes sure your proteins behave—kind of like the old-fashioned chaperone that escorted you and your boyfriend to the movies,” Dr. Cuervo says.
CMA becomes less efficient as people age, increasing the risk that unwanted proteins will form insoluble clumps that accumulate and ultimately damage the brain’s neurons. Evidence has shown that abnormal copies of a particular protein called tau clump together within neurons to form protein tangles that contribute to Alzheimer’s.
To investigate the role of impaired CMA in Alzheimer’s, Dr. Cuervo and her colleagues genetically engineered mice to possess brain neurons that lacked CMA. The absence of CMA in those brain cells was enough to cause short-term memory loss, impaired walking, and other problems often found in rodent models of Alzheimer’s disease.
Was CMA loss linked to human Alzheimer’s as well? To find out, the researchers studied brain neurons retrieved postmortem from Alzheimer’s patients and from a comparison group of healthy individuals, obtaining single-cell RNA-sequencing data to calculate CMA’s activity level. Sure enough, CMA activity was somewhat inhibited in people who had been in the early stages of Alzheimer’s, followed by much greater CMA inhibition in the brains of people with advanced Alzheimer’s.
In an encouraging finding published in Cell in 2021, Dr. Cuervo reported that a novel drug, called CA, shows potential for treating Alzheimer’s by revving up CMA. When tested in two different mouse models of Alzheimer’s disease, oral doses of CA given over the course of four to six months led to improvements in memory and decreases in depression and anxiety that made the treated animals resemble healthy control mice. CA was developed by Dr. Cuervo in collaboration with her research colleague Evripidis Gavathiotis, Ph.D., professor of biochemistry and of medicine at Einstein.
“We know that CMA is capable of digesting defective tau and other proteins,” Dr. Cuervo says. “But the sheer amount of defective tau in Alzheimer’s overwhelms CMA and essentially cripples it. Our drug revitalizes CMA efficiency by boosting levels of a key CMA component.”
Drs. Cuervo and Gavathiotis have teamed up with Life Biosciences of Boston, Mass., which is developing CA and related compounds for treating Alzheimer’s and other neurodegenerative diseases.
Who among us hasn’t forgotten a friend’s name or where we left our car keys? For those of a certain age, memory lapses could be benign “senior moments” or signs of predementia—the early stage of dementia, when individuals can still engage in daily activities but are at risk for developing full-blown dementia.
Telling the difference between harmless and harmful memory issues requires time-consuming and expensive clinical workups and brain imaging that may not yield clear-cut results. That uncertainty makes it hard for seniors to plan for the years ahead, for doctors to know whether to intervene, and for researchers to devise and evaluate new therapies to prevent or slow cognitive decline.
Now, thanks to the work of an Einstein scientist, predementia can be detected—and the risk for developing dementia predicted—using a test that takes just a minute or so and costs practically nothing.

As a young researcher, I had examined hundreds of patients and noticed that if an older person was walking slowly, there was a good chance that his or her cognitive tests would also be abnormal.
—Dr. Joe Verghese
“As a young researcher, I had examined hundreds of patients and noticed that if an older person was walking slowly, there was a good chance that his or her cognitive tests would also be abnormal,” explains Joe Verghese, M.B.B.S., M.S., director of the Montefiore Einstein Center for the Aging Brain, professor in the Saul R. Korey Department of Neurology, and the Murray D. Gross Memorial Faculty Scholar in Gerontology at Einstein. “This gave me the idea that perhaps we could use this simple clinical sign—how fast someone walks—to predict who would develop dementia.”
He ultimately devised a test that measures patients’ gait speed and also asks about cognitive complaints. Slow gait combined with cognitive problems would constitute what Dr. Verghese calls motoric cognitive risk syndrome (MCR), a new way of characterizing predementia.
To evaluate the usefulness of testing for MCR, Dr. Verghese and colleagues assessed MCR in nearly 27,000 adults from 17 countries who were ages 60 and over and were dementia-free at the time. About one in 10 tested positive for predementia—and, over the next 12 years, those people were twice as likely as the other participants to develop dementia. The results were published in 2014 in the journal Neurology.
“Our method enables many more people to learn if they’re at risk for Alzheimer’s, since the test doesn’t need to be administered by a neurologist,” Dr. Verghese said at the time. “The payoff could be tremendous—not only for individuals and their families, but also in terms of healthcare savings for society.”
Some patients testing positive for MCR, says Dr. Verghese, may have treatable conditions (hypertension, smoking, high cholesterol, obesity, or diabetes, for example) that increase the risk for dementia by interfering with blood flow to the brain. As for those who meet MCR criteria but have no treatable underlying health issues: “Even in the absence of a specific cause, we know that healthy lifestyle factors, such as exercising and eating healthier, can reduce the rate of cognitive decline,” Dr. Verghese says. “Our group has also shown that cognitively stimulating activities—playing board games and card games, reading, writing, and also dancing—can delay dementia’s onset.”
In a new study funded by a five-year, $7.6 million NIA grant, Dr. Verghese and his colleagues are seeking to determine the biological roots of MCR and identify biomarkers for the condition. The research involves 11,000 older adults enrolled in eight ongoing international studies of aging.
Dr. Verghese’s team also wants to identify the brain structures involved in MCR and learn how they change over time—research led by Helena Blumen, Ph.D., M.S., an associate professor of medicine and in the Saul R. Korey Department of Neurology at Einstein.
 Helena M. Blumen, Ph.D., works with a woman as part of a study contrasting the cognitive and brain benefits of treadmill walking and social ballroom dancing.
Helena M. Blumen, Ph.D., works with a woman as part of a study contrasting the cognitive and brain benefits of treadmill walking and social ballroom dancing.
In previous studies using magnetic resonance imaging, Dr. Blumen found that MCR was associated with a widespread pattern of cerebral-cortex atrophy in regions associated with motor control, social behaviors, cognition, and affective functions (e.g., emotions).
“We’ve already uncovered clues suggesting that MCR is distinct from other predementia conditions, and now we can dig deeper to refine our understanding of this syndrome,” says Dr. Verghese. “We hope to identify new ways to prevent or treat MCR and slow or stop its progression to Alzheimer’s.”

We hope to find ways to intervene that may promote brain health and prevent cognitive decline.
—Dr. Carol Derby
Since 1980, NIH grants have supported the long-running Einstein Aging Study (EAS), which focuses on the aging brain. The EAS examines both normal aging and the challenges posed by Alzheimer’s disease and other dementias and so far has studied more than 2,500 Bronx residents age 70 and older. Current EAS participants are 40% non-Hispanic Black, 46% non-Hispanic white, and 13% Hispanic.
“We have a major focus on health equity,” says Richard B. Lipton, M.D., who has led the EAS since 1992. “Recent and ongoing studies have looked at race, ethnicity, neighborhood deprivation, and perceived discrimination as risk factors for cognitive decline and for the development of Alzheimer’s and other dementias.”
Assessing potentially modifiable risk factors for dementia is an EAS priority. Its 2016 study in Alzheimer’s Disease & Associated Disorders found that feeling stressed increases the likelihood that elderly people will develop mild cognitive impairment—often a prelude to full-blown Alzheimer’s disease. And its 2019 study in Current Alzheimer’s Research found that pain that interferes with daily activities is associated with increased risk for developing dementia.
 Richard B. Lipton, M.D., examines a Bronx resident and participant in the long-running Einstein Aging Study.
Richard B. Lipton, M.D., examines a Bronx resident and participant in the long-running Einstein Aging Study.
“Chronic pain affects about half of adults over age 70, and these findings suggest that better pain treatment in older adults may reduce the risk for cognitive decline,” says Dr. Lipton, who is a professor in the Saul R. Korey Department of Neurology, of psychiatry and behavioral sciences, and of epidemiology & population health, and the Edwin S. Lowe Chair in Neurology at Einstein, as well as vice chair of neurology at Einstein and Montefiore.
For the past five years, the EAS has taken advantage of smartphones to gain unprecedented insights into the aging brain. “In the past, we assessed cognition exclusively through in-person tests in our clinical laboratory,” says Mindy Joy Katz, M.P.H., senior associate in the Saul R. Korey Department of Neurology and the EAS project coordinator. “By adding smartphones, we’re able to bring measures of cognitive performance directly to the community.”
Taking frequent measures over many days rather than isolated lab readings “gives us a truer sense of a person’s cognitive [thinking] abilities and how those abilities change from day to day in the course of their daily lives,” Ms. Katz says. “These methods have allowed us to follow people throughout the pandemic, when in-person visits aren’t safe.”
A recently announced five-year, $32 million renewal grant from the National Institutes of Health will fund the EAS and its smartphone program, which is co-led at Einstein by Dr. Lipton and Carol Derby, Ph.D. The program will follow more than 750 Bronx adults, who will receive customized smartphones as well as special watches for assessing their cognitive ability several times a day over two weeks.
Participants will respond on their phones to memory challenges or brain games. At the same time, they’ll respond to prompts asking about conditions that may be affecting their thinking ability, including sleep quality, stress, pain, air pollution, and regulation of blood-glucose levels.
“Once we have these detailed, real-time measures of risk factors that can be modified, we hope to find ways to intervene to promote brain health and prevent cognitive decline,” says Dr. Derby, who is a research professor in the Saul R. Korey Department of Neurology and of epidemiology & population health and the Louis and Gertrude Feil Faculty Scholar in Neurology at Einstein.
90% of the more than 11 million caregivers who watch over dying elders in the United States yearly are unpaid; most are unprepared for the role.
Unfortunately, few of these studies will yield therapies for the current generation of Alzheimer’s patients and their families. An average of 12 years is required for a drug to work its way through the approval process—and the vast majority of experimental drugs never make it to market because the drugs are deemed ineffective or have intolerable side effects.
“We have cured Mouseheimer’s over and over, [but] we have trouble translating the work to humans,” Dr. Verghese says in the book Dementia Reimagined, written by Einstein’s Tia Powell, M.D., whose grandmother and mother succumbed to dementia.
In her book Dr. Powell makes an impassioned plea for the healthcare industry to focus more of its efforts on the here and now—on care as well as cure. “The standard argument for spending money on drug research is that we must win this battle or we’ll face unbearable expenses caring for the millions who will develop dementia as our population ages,” says Dr. Powell, who is a professor of epidemiology & population health and of psychiatry and behavioral sciences and the Dr. Shoshanah Trachtenberg Frackman Faculty Scholar in Biomedical Ethics at Einstein. She is also the director of the Montefiore Einstein Center for Bioethics. “But that awful situation is already here. With no cure in sight, we can no longer neglect the millions whose comfort should be supported through better palliative treatment.”
With no cure in sight, we can no longer neglect the millions whose comfort should be supported through better palliative treatment.
—Dr. Tia Powell
Dr. Powell notes that 90% of the more than 11 million caregivers who watch over dying elders in the United States yearly are unpaid; most are unprepared, technically or psychologically, for that role. “We ignore caregivers and what they do for people at our peril,” she says. “They are the safety net and the key to living with dementia.”
Dr. Powell’s take on Alzheimer’s isn’t entirely pessimistic, as noted by her book’s subtitle, Building a Life of Joy and Dignity from Beginning to End. “Having dementia or seeing a loved one suffer from it can be lousy, as millions of people across the globe can attest—but it is not always so,” she says. “Although certain aspects can’t be eliminated, they can be diminished and compressed, making the experience less lousy for everyone.”
The final chapter of Dementia Reimagined is rich with practical insights for patients and caregivers, gleaned from Dr. Powell’s professional and personal experience with Alzheimer’s patients, such as:

If Dr. Powell’s recommendations were incorporated into a clinical program, it would resemble the Montefiore Hudson Valley Center of Excellence for Alzheimer’s Disease (CEAD). The CEAD is part of a network of 10 centers established in 2016 by the New York State Department of Health. Its purpose: to make early screening and diagnosis of dementia more widely available, support research into causes and potential treatments, expand the expertise of the healthcare workforce, and provide better access to community-based services for patients and their caregivers.
Montefiore’s CEAD leverages the expertise of the Center for the Aging Brain and the Memory Disorders Center. The CEAD is staffed by neurologists, geriatricians, psychiatrists, neuropsychologists, and social workers who collaborate to provide patients and their families with cost-effective services, including treatment, counseling, education, referrals to support programs, and access to clinical trials. Crucially, it recognizes the reality that day-to-day dementia care almost always falls to a spouse, child, or other close relative.

I developed Montefiore’s CEAD with my own family in mind and vowed it would focus on the patient and the caregiver.
—Dr. Jessica Zwerling
“I developed Montefiore’s CEAD with my own family in mind and vowed it would focus on the patient and the caregiver,” says Jessica Zwerling, M.D., M.S., director of the CEAD, associate director of the Montefiore Einstein Center for the Aging Brain, and clinical director of the Einstein Aging Study. “Caregivers are an especially vulnerable population, with higher rates of stress, depression, and cognitive impairment themselves. My grandmother had Alzheimer’s, and my uncle had a heart attack from the stress of caring for her.”
Dr. Zwerling, who is also an associate professor in the Saul R. Korey Department of Neurology and an assistant professor of pediatrics and of psychiatry and behavioral sciences at Einstein, sums up her model of dementia care as including what she calls the “Five Cs”: Culturally competent, collaborative care of the cognitively impaired older adult. Attaining cultural competence—understanding the community—can be particularly challenging: So far, CEAD staffers have conducted Alzheimer’s screenings in 17 different languages, reflecting the diversity of the population that the center serves throughout the seven counties of the Hudson Valley.
The Montefiore-Einstein model of dementia care was described in a 2016 paper in the Journal of the American Geriatrics Society. It has since been replicated at a number of other institutions.
My father probably received the best care possible. And thanks to my parents’ resources, my mom was able to bridge the yawning gaps in insurance coverage and still have a nest egg for her retirement. But as Dr. Powell has written, “Money helps with some things, but nothing removes the sting of watching a loved one become someone you don’t know.”
During his final two years, my father needed assistance with every aspect of daily living. He spoke little and idled away the hours at home in front of a big-screen TV, drifting in a sea of disconnected thoughts and old memories, with occasional moments of confusion and agitation.
“The last phase may persist a year or more,” Dr. Powell says. “That whole final year is what we need to fix to arrive at a good death.”
Those last months were indeed unsettling. In early 2008, my father collapsed in the shower, breaking his hip. His doctors recommended joint-replacement surgery to stabilize his hip and dampen the searing pain. (He had long since lost the ability to walk.) He came home after a few weeks spent recovering in a nursing home. But almost every trace of the parent, provider, and protector I once knew had vanished.
After one last health crisis and one more hospital stay, nothing could be done except to take him home for his final days. We withdrew food and water and comforted him with drops of morphine. Still, he lingered for almost a week, passing away early on the morning of my parents’ 58th wedding anniversary.
Like others who have lost a parent to Alzheimer’s, I worry about my own cognitive health in the years ahead, especially since I take after my father in many ways. In the meantime, I’ll heed Dr. Powell’s advice: take walks, spend time with loved ones, work to increase my store of happiness … and hope that Einstein and Montefiore’s promising Alzheimer’s research bears fruit.
In a prospective study of 542 community-dwelling seniors, Mirnova Ceide, M.D., M.S., and colleagues found that apathy predicted motoric cognitive risk syndrome—a form of predementia first described by Einstein researchers, in which older adults have an abnormally slow gait and cognitive complaints. The findings, published in 2020 in the Journal of Gerontology, Series B: Psychological Sciences and Social Sciences, suggest that treating apathy might forestall the onset of disabilities related to dementia. Dr. Ceide is an assistant professor of psychiatry and behavioral sciences and of medicine at Einstein and a psychiatrist at Montefiore.
Einstein investigators have developed a five-minute cognitive screening (5-Cog) to identify people at high risk for developing dementia. The 5-Cog screen was designed to overcome the logistical, educational, and cultural barriers inherent in existing cognitive screening tools, according to Erica F. Weiss, Ph.D., one of the investigators. The Einstein team is currently evaluating 5-Cog on 1,200 patients in a clinical trial funded by the National Institute of Neurological Disorders and Stroke. Dr. Weiss is the associate director of neuropsychology at the Montefiore Center for the Aging Brain and an assistant professor in the Saul R. Korey Department of Neurology at Einstein.
Einstein researchers are evaluating an at-home version of transcranial direct current stimulation (tDCS) for treating Alzheimer’s. A painless, noninvasive therapy, tDCS delivers low-intensity electric current to the brain using a fitted headband. It has improved cognitive performance in animals and in limited human studies, reports Helena Knotkova, Ph.D., D.Phil., a co-leader of the study. The therapy is being tested on 100 patients with mild to moderate Alzheimer’s in a five-year, $6.2 million study funded by the National Institute on Aging. Dr. Knotkova is a professor of family and social medicine at Einstein and the director of clinical research at the MJHS Institute for Innovation in Palliative Care, an Einstein affiliate.
To find gene variants that contribute to longevity, Zhengdong Zhang, Ph.D., and colleagues conducted the largest whole-exome sequencing study of centenarians to date. (The exome is the part of the genome that codes for proteins.) Rare coding variants in the Wnt signaling pathway had a prolongevity effect in those centenarians possessing APOE4, a well-known, common gene variant associated with risk for Alzheimer’s and other age-related conditions. The results, reported in 2021 in Nature Aging, suggest that the Wnt-signaling gene variants counteract the adverse health effects associated with the APOE4 gene. Drugs designed to mimic the effects of those protective Wnt-signaling variants may benefit people with the APOE4 gene variant, and possibly others. Dr. Zhang is a professor of genetics at Einstein.
Yasmin Mossavar-Rahmani, Ph.D., R.D., is testing whether a diet featuring foods with anti-inflammatory properties can reduce cognitive decline and Alzheimer’s disease risk. The dietary pattern was crafted to appeal to a multicultural population and is being tested on about 300 adults from Co-op City (a large and diverse north Bronx neighborhood) and nearby communities. The study is funded by a five-year, $4 million grant from the National Institutes of Health. Dr. Mossavar-Rahmani is a professor of epidemiology & population health at Einstein.
* Joe Verghese, M.B.B.S., M.S., director of the Montefiore Einstein Center for the Aging Brain, is also a principal investigator on these research projects.