When William Southern, M.D. ’92, M.S., chief of hospital medicine in the department of medicine at Einstein and Montefiore, introduces himself to new patients, the conversation often goes like this:
“Hello, Mr. Brown, I’m Dr. William Southern, your hospitalist.”
“Nice to meet you, Dr. Southern. Where’s my doctor?”
“I’ll be taking care of you while you’re in the hospital.”
“OK, but where’s my doctor?”
 Shitij Arora, M.B.B.S., left, and internal medicine resident Lindor Qunaj, M.D., attend to a patient at Montefiore's Moses campus.
Shitij Arora, M.B.B.S., left, and internal medicine resident Lindor Qunaj, M.D., attend to a patient at Montefiore's Moses campus.
Unless you or a loved one has been hospitalized in the last decade or so, you may have missed a profound medical shift: the takeover of inpatient care by hospitalists—physicians who specialize in caring for hospitalized patients.
Several factors have fueled the hospitalist revolution. Hospitalized patients suffer from increasingly complex health problems, and their primary-care physicians are busier than ever in the clinic and don’t have time to provide the care that inpatients need. In addition, managed care incentivizes hospitals to discharge patients as quickly as possible, putting a premium on clinicians with inpatient-specific skills and experience. Finally, rules that now limit residents’ time on the wards mean that extra staff members—today’s hospitalists—are needed for inpatient care.
You build intense relationships with patients and their families, seeing them multiple times a day, every day. It’s incredibly rewarding.
— Dr. William Southern
Dr. Southern’s own career mirrors this revolution in healthcare. “When I finished my residency in medicine in 1995, I took a job at Mount Sinai Hospital [in Manhattan] taking care of patients who were being admitted to the hospital,” he says. “The medicine service—primarily medical school faculty responsible for both clinical care and teaching—couldn’t handle the growing caseload, a common story at many teaching hospitals. So they hired physicians exclusively focused on patient care, and I was one of them.”
He had found his calling. “You’re under pressure to make key decisions when working with such sick patients,” Dr. Southern says. “But you build intense relationships with patients and their families, seeing them multiple times a day, every day. It’s incredibly rewarding.”
Most hospitalists are physicians who have completed a residency in internal medicine, emergency medicine, family medicine, or pediatrics—some of which have special tracks that can lead to careers as hospitalists.
For example, the Einstein and Montefiore internal medicine residency program offers a Hospital Medicine and Health System Pathway, which prepares physicians to become hospital-based clinicians. In addition, the American Board of Internal Medicine and the American Board of Family Medicine provide certifications to their board-certified physicians who have attained specialized knowledge and skills in hospital medicine, which is not yet a board-certified specialty itself when it comes to caring for adult patients. However, in 2015, the American Board of Pediatrics recognized pediatric hospital medicine as a pediatric specialty, and so did the American Board of Medical Specialties in 2016. In 2019, the first pediatric hospital medicine board exam was given to more than 1,400 applicants.
Dr. Southern became a hospitalist before the term was coined. That happened with the 1996 publication of “The Emerging Role of ‘Hospitalists’ in the American Health Care System,” in The New England Journal of Medicine (NEJM). Authors Robert M. Wachter, M.D., and Lee Goldman, M.D., M.P.H., of the University of California, San Francisco, the unofficial birthplace of hospital medicine in the United States, predicted “the rapid growth of a new breed of physicians we call ‘hospitalists’ … who will be responsible for managing the care of hospitalized patients in the same way that primary-care physicians are responsible for managing the care of outpatients.”
“People like me excitedly forwarded the article to our peers, since this is what we were doing,” Dr. Southern says. “I could see the potential for a career as a hospitalist taking shape.”
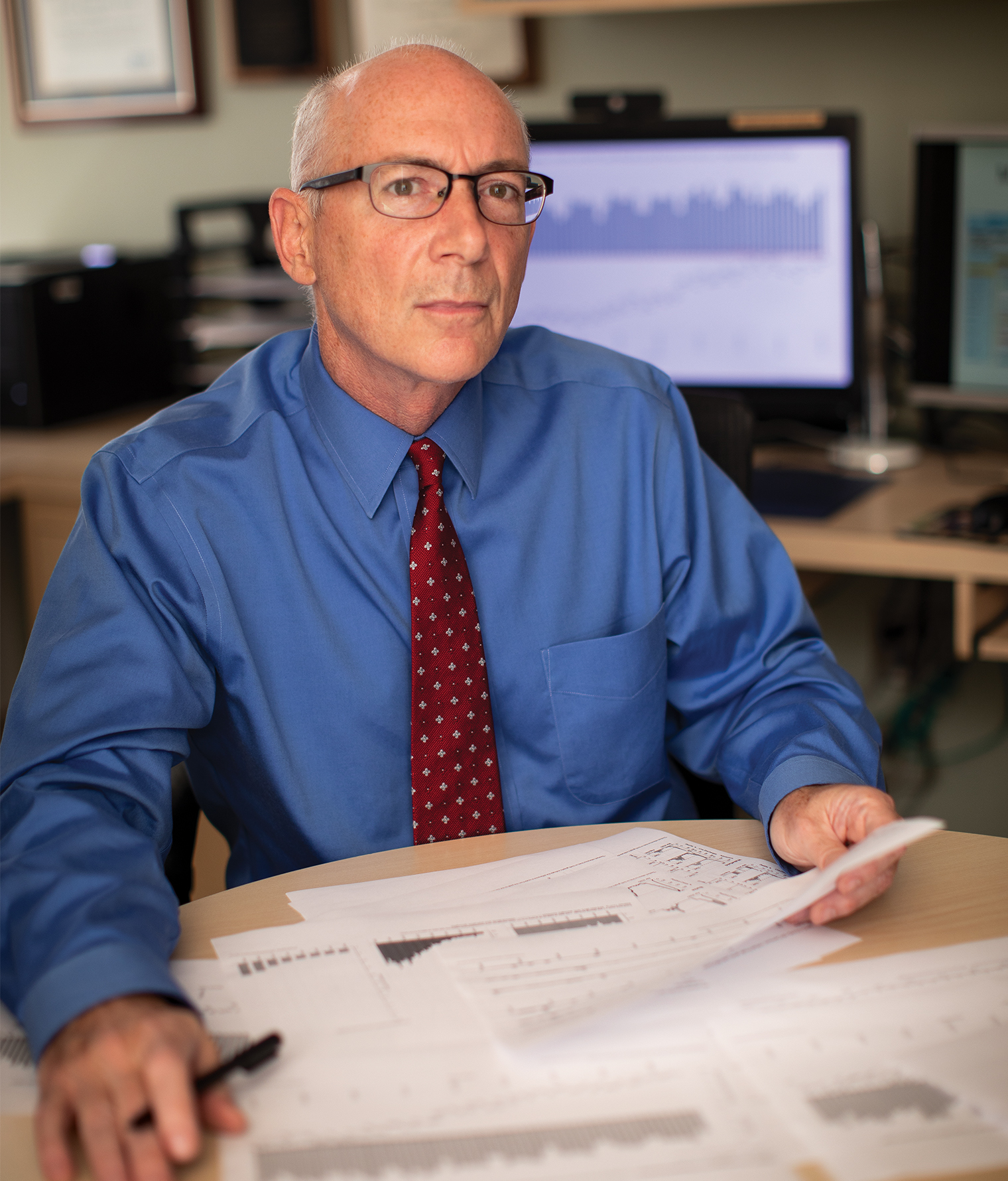 Dr. William Southern, chief of hospital medicine in the department of medicine at Einstein and Montefiore, became a hospitalist before the term was even coined.
Dr. William Southern, chief of hospital medicine in the department of medicine at Einstein and Montefiore, became a hospitalist before the term was even coined.
Specialists still see many inpatients in this new paradigm of care. However, hospitalists assume responsibility for developing a comprehensive care plan and ensuring that patients in the hospital receive services in a timely and efficient manner.
Hospital medicine caught on with stunning speed, reshaping inpatient care and medical education. From a few hundred in the 1990s, the number of hospitalists has grown to about 60,000 today, making it the third-largest specialty after general internal medicine and family medicine. A 2015 Association of American Medical Colleges survey found that half of all recent graduates who intended to specialize in internal medicine planned to work as hospitalists. They can now be found in about three-quarters of American hospitals, including all top-tier medical centers.
Montefiore was an early adopter. It began hiring hospitalists at the start of the 2000s and now has 102 on staff. They oversee 175 full- and part-time physician assistants and manage 839 beds across Montefiore Medical Center’s three campuses (Moses, Weiler, and Wakefield).
It was an extraordinarily bold step born of necessity. It’s still the most meaningful treatment we give to COVID-19 patients with high levels of inflammation.
— Dr. William Southern
Twenty-five years on, Dr. Southern must still explain his role to patients. “It’s jarring for some patients to learn that their primary-care physician isn’t there [in the hospital] for them,” he acknowledges. “One of our jobs is managing that concern. I always tell patients how they stand to benefit from my expertise in caring for complex cases and from my ready availability. If they have concerns, I can be at their bedside in minutes, rather than having them wait for their primary-care doctor to call or drop by the next day. I think people totally get that.”
Indeed, numerous studies show that the rise of hospital medicine has not affected patient satisfaction or quality of care, while at the same time it has cut healthcare costs and lengths of stay.
“Let me tell you a story about what happened here at the beginning of the pandemic,” Dr. Southern adds. “Our population of COVID-19 patients was doubling every two days, and many of them were very sick and deteriorating. At the time, there were no proven therapies for the disease. Fortunately, we had a staff that was able to handle this deluge. One of those people deserves special mention.”
Dr. Southern was referring to Shitij Arora, M.B.B.S., associate professor of medicine at Einstein and a hospitalist at Montefiore, whom he describes as “an extraordinary clinician, the kind of doctor whom other doctors ask for advice.”
Dr. Arora’s tale began early in the pandemic, in March 2020, when a middle-aged Bronx woman was admitted to Montefiore in acute respiratory distress due to COVID-19, and Dr. Arora was her doctor. Since the patient’s oxygen requirements were extremely high, Dr. Arora called for a high-flow oxygen system—but learned that none would be available for several hours. Standard procedure called for putting her on a mechanical ventilator instead, “but I knew that if we intubated her, her chances of surviving would be very low,” he recalls.
A blood test had shown that the patient’s inflammation level was extremely elevated. So Dr. Arora prescribed a corticosteroid—contradicting the guidelines of two prominent clinical organizations (the Infectious Diseases Society of America and the Society of Critical Care Medicine), which recommended against using steroids on COVID-19 patients.
Those guidelines were based on limited data from treating patients sickened by MERS and SARS, two similar coronavirus-caused respiratory diseases. However, Dr. Arora’s experience and instincts told him that patients like the Bronx woman, whose lungs exhibited signs of over-the-top inflammation (the feared “cytokine storm”), would benefit from an anti-inflammatory drug. “It was an extraordinarily bold step born of necessity,” Dr. Southern says.
Within hours, the woman’s condition improved dramatically, and she was discharged after five days in the hospital. Dr. Arora ordered the same steroid treatment for four other severely ill COVID-19 patients—all with low blood-oxygen readings and high levels of inflammation—and all recovered. It soon became standard protocol for certain patients at Montefiore and other hospitals.
“It’s still the most meaningful treatment we give to COVID-19 patients with high levels of inflammation,” Dr. Southern says.
A few months later, Dr. Arora’s approach was vindicated by Britain’s RECOVERY trial, the first large-scale, randomized test of the steroid dexamethasone in patients hospitalized with COVID-19. As described in NEJM, the British trial found that steroid use reduced mortality by one-third in those receiving mechanical ventilation and by one-fifth in those receiving oxygen support without ventilation. Around the same time, Dr. Arora and his colleagues came to the same conclusion with a study of their own. (See “Which COVID-19 Patients Are Most Likely to Benefit From Steroids,” below.)
“This is why you want a hospitalist in charge of your care,” Dr. Southern says.
Shitij Arora, M.B.B.S., associate professor of medicine at Einstein and a hospitalist at Montefiore, had shown that steroids could help in treating Montefiore patients who were severely ill with COVID-19—a finding confirmed by Great Britain’s RECOVERY trial. But which patients are most likely to benefit? Could some be harmed by it?
To answer those questions, Marla Keller, M.D., vice chair for research in the department of medicine at Einstein and Montefiore, William Southern, M.D., M.S., chief of hospital medicine in the department of medicine at Einstein and Montefiore, Dr. Arora, and colleagues carried out an observational study of 1,946 COVID-19 patients, 140 of whom had been treated with glucocorticoids (a class of steroid hormone) within 48 hours of hospital admission and a control group of 1,666 similar patients who were not given steroids.
The study found that in patients with a high level of inflammation (indicated by elevated levels of C-reactive protein, which the liver produces in response to inflammation), steroid treatment reduced the risk of mortality or the need for mechanical ventilation by 75%. However, in COVID-19 patients with low levels of inflammation, steroid treatment more than doubled the risk of mortality and need for ventilatory support, the researchers reported in August 2020 in the Journal of Hospital Medicine.
“Steroids are very powerful drugs and not appropriate for all COVID-19 patients,” Dr. Arora says. “It’s just as important to avoid giving steroids to patients who may be harmed as it is to give steroids to those who may benefit. Our study suggests that the simple and inexpensive blood test for C-reactive protein can help determine which patients will benefit from these drugs.”
When Dr. Southern began his career, hospitalists were hired almost exclusively to fill gaps in inpatient care. While “direct-care” hospitalists still dominate the field, more and more hospitalists are finding careers in academic medicine—a trend that Drs. Wachter and Goldman envisioned back in 1996.
Hospitalists, they wrote, would fit neatly into the academic enterprise, where “a premium will be placed on clinical quality improvement, the development of practice guidelines, and outcomes research, not only to provide the physician with a creative outlet and a potential source of funding during the nonclinical months but also to give the academic center a practical research-and-development arm.”
At Einstein and Montefiore, the academic hospitalist model blossomed in 2011, when the department of medicine created a division of hospital medicine, allowing hospitalists to pursue interests such as research and teaching in addition to inpatient care. Dr. Southern, the division’s founding chief, notes that hospital administrators elsewhere haven’t always immediately seen the value of academic hospitalists.
“Many hospital administrators want clinicians who will see patients and focus mainly on quality of care and efficiency—the business model that underpins hospital medicine,” he says. “My view is that we can’t have 15% turnover per year, with our best hospitalists leaving for fellowships or other opportunities for career advancement. To reap the benefits of having these expert clinicians and to retain them requires engaging them in the academic enterprise. In fact, when I’m recruiting hospitalists, one of our greatest selling points is offering them the chance to teach, do research, and find leadership positions in the hospital along with taking care of patients.”
I interviewed at many places in New York City and chose Montefiore because of the teaching opportunities.
— Dr. Allison Ludwig
Teaching Opportunities
Many hospitalists double as teachers—a dual role that has changed undergraduate and graduate medical education. “In the past, teaching was primarily conducted by specialists or subspecialists, who would spend a month or two each year attending on the wards,” says Todd Cassese, M.D., professor of medicine and associate dean for medical education at Einstein and a hospitalist at Montefiore. “They were good at teaching and caring for patients affected by diseases in their areas of expertise but weren’t necessarily equipped with the breadth of expertise to manage the increasing number of seriously ill patients with multiple health problems.”
In their 1996 NEJM article, Drs. Wachter and Goldman predicted that the rise of hospital medicine would make it more likely for residents to be “supervised by attending physicians who are highly skilled and experienced in providing inpatient care … [and] answer public calls for closer and more effective faculty oversight of house staff and students.” That has certainly proved to be the case at Einstein and Montefiore, where the opportunity to teach as well as care for patients has helped lure hospitalists.
“I interviewed at many places in New York City and chose Montefiore because of the teaching opportunities,” says Allison Ludwig, M.D. ’04, associate professor of medicine and associate dean for student affairs at Einstein and now a hospitalist at Jacobi Medical Center.
Dr. Southern began nurturing a select group of teaching hospitalists in 2011. With their patient load slightly reduced, they devote most of their time to leading teaching teams and mentoring medical students and residents—a staffing pattern seen at fewer than one-third of teaching hospitals. “For these clinicians, teaching is not just part of the job,” he says. “It’s the core of their job, and the expectation is that they do it well. Clinically, it’s the happiest I’ve ever been,” adds Dr. Southern, a teaching hospitalist himself. “It’s amazing to be able to give so much time to patients and to learners.”
Einstein’s medical students get their first exposure to hospital medicine during years one and two, in the Introduction to Clinical Medicine course, where the preceptor is likely to be a hospitalist. Their next and most intense hospital medicine experience comes in year three, during the six-week internal medicine clerkship, in which hospitalists lead most of the teaching teams at the hospital sites. In their fourth year students may take a one-month internship where they serve on direct-care teams and work directly with hospitalists, without interns and residents.
 Todd Cassese, M.D., professor of medicine and associate dean for medical education at Einstein and a hospitalist at Montefiore, instructs a class at Einstein.
Todd Cassese, M.D., professor of medicine and associate dean for medical education at Einstein and a hospitalist at Montefiore, instructs a class at Einstein.
“I didn’t know much about hospital medicine until my internal medicine clerkship,” says Brett Fischer, M.D., who graduated from Einstein in 2015 and is now a hospitalist at Weill Cornell Medicine in Manhattan. Like many of his peers, Dr. Fischer considered training for a subspecialty.
As medical school went on, however, he found himself drawn to the breadth and depth of hospital medicine. “The nature of medical education is to focus on organ systems and the underlying physiology,” he says. “While I loved learning all of that, I preferred to concentrate on the big picture—on taking care of the whole patient.”
Dr. Fischer also developed a liking for evidence-based medicine, which he first encountered at Einstein in the required preclinical Epidemiology, Population Health, and Evidence-Based Medicine course, led by Robert Goodman, M.D., associate professor of medicine at Einstein and a hospitalist at Montefiore. “In my clerkships and subinternships, in which I worked right alongside hospitalists, I loved seeing how evidence-based medicine was practiced in the real world, and I wanted to emulate that,” Dr. Fischer says. He now teaches the subject to medical students at Weill Cornell.
Hospital medicine also figures prominently in Einstein and Montefiore’s internal-medicine residency. During the third year, residents can select a hospital-medicine pathway. Immersed in the role of direct-care hospitalist, they participate in hospital-wide committees, work with leaders in the field, and conduct scholarly projects, preferably in quality improvement.
One concern about hospitalists as teachers is that students “may not connect with specialists doing cutting-edge basic-science research and thus be less likely to become physician-scientists,” Dr. Cassese says. “As part of the latest curriculum renewal, we’re integrating basic-science learning experiences into the clinical years, to expose students to the science and the scientists who might spark career interests.”
 Trina Dhar, M.D., internal medicine clerkship site director at Weiler Hospital, goes over patient care with her team, from left: Einstein third-year medical student Faraz Sewani, Einstein fourth-year medical student Christopher Itua, and first-year resident Adam Haines, M.D.
Trina Dhar, M.D., internal medicine clerkship site director at Weiler Hospital, goes over patient care with her team, from left: Einstein third-year medical student Faraz Sewani, Einstein fourth-year medical student Christopher Itua, and first-year resident Adam Haines, M.D.
Clinical Research Opportunities
Hospitalists spend more time at the bedside than most physicians do, so conducting clinical research makes a lot of sense. “We’re ideally positioned to ask how care can be improved,” Dr. Southern says. “Our COVID-19 steroid study is a perfect example of that.” He started conducting research himself about a decade ago after completing Einstein’s Clinical Research Training Program, which gives practicing physicians all the tools they need to engage in rigorous scientific inquiry.
In one of his first projects, Dr. Southern investigated wrong-patient orders in electronic health record (EHR) systems and how to prevent them. His research showed that such errors are much more common than previously thought (occurring thousands of times a year even at the best institutions). Requiring providers to reenter patient identifiers into a health record when placing an order reduced wrong-patient orders by 41%, he reported in 2010 in the Journal of the American Medical Informatics Association.
More recently, Dr. Southern led a study asking if patient safety is compromised when physicians are allowed to open EHRs for several patients at once—a practice that hospitals typically bar, to reduce the chance of mix-ups. Many clinicians, however, believe the practice improves productivity without compromising safety. Dr. Southern’s study, published in 2019 in the Journal of the American Medical Association, found that wrong-patient orders did not increase even when physicians were allowed to open up to four EHRs simultaneously.
Another hospitalist-researcher is Cristina Gonzalez, M.D. ’04, professor of medicine, who studies whether implicit, or unconscious, bias influences physician behaviors when they communicate with patients or make medical decisions. (Learn more about Dr. Gonzalez’s work.)

One challenge in hospital medicine is making sure that the transition in care from the community-based physician to the hospitalist goes smoothly.
“In the traditional model, the same doctors who’d cared for patients over months or years would be caring for them in the hospital—which no longer happens with hospital medicine,” says William Southern, M.D., M.S., chief of hospital medicine in the department of medicine at Einstein and Montefiore. “Some would say that’s bad for patients. At perhaps the most critical moment in their lives, when most in need of a trusted physician, they get someone they’ve never met before.”
Todd Cassese, M.D., professor of medicine and associate dean for medical education at Einstein and a hospitalist at Montefiore, agrees. “When the patient enters the hospital, the hospitalist doesn’t know what the primary-care doctor knows—which can be dangerous if communication is lacking.” Dr. Cassese says. “But many healthcare systems are finding solutions with better use of electronic health record systems and other technological and procedural fixes.”
Matthew Shaines, M.D., associate professor of medicine and a Montefiore hospitalist for 15 years, has this to say about patient handoffs: “Transitions in care can be significant sources of medical errors. So as patients get closer to discharge, we as hospitalists need to make sure that their personal physicians—who care for these patients both before and after our involvement—are well briefed on their condition and the care they might require going forward.”
An even greater challenge for the hospitalist arises when there’s no handoff on either side of the hospital stay—a common scenario at urban hospitals, where many patients have no personal physicians.
“There’s a sizable group of patients here who use the emergency department for regular care,” says Tulay Aksoy, M.D., assistant professor of medicine at Einstein and medical director of the Wakefield campus. “We try to care for them as if we’re their primary-care providers and direct them to the appropriate care upon discharge.”
My various roles in hospital medicine have given me a good perspective on how the whole hospital works and how we can help people across the Montefiore Health System.
— Dr. Jessica Dekhtyar
Administrative Opportunities
Jessica Dekhtyar, M.D. ’09, assistant professor of medicine at Einstein and a hospitalist at Montefiore, didn’t intend to become a leader in the hospital, or even a hospitalist. But during her residency in medicine at Montefiore, she found that she liked the intensity and complexity involved in caring for inpatients, as well as the social and collaborative environment that hospital medicine offered.
After joining the Montefiore staff in 2012, she involved herself in quality-improvement projects, working with nursing, patient logistics, and environmental services. She was soon appointed unit medical director of Northwest 8 (one of 10 medicine units at the Moses campus), a role requiring even wider collaboration. In 2014, she was tapped to become director of medical services on the Moses campus, where she oversees 40 hospitalists, quality and safety activities, hospitalist recruitment and retention, and the teaching service.
While still seeing patients, Dr. Dekhtyar is now medical director of Montefiore’s Transfer Center, which involves coordinating the transfer of acutely ill patients from smaller satellite hospitals to the Moses campus, the network’s hub for advanced medical care.
“My various roles in hospital medicine have given me a good perspective on how the whole hospital works and how we can help people across the Montefiore Health System,” she says.
A growing trend among hospitalists is to work with specialists in co-managing particular types of patients. For example, the Children’s Hospital at Montefiore started a pediatric hospital medicine service in 2007 and is now home to the largest group of child-focused hospitalists in the tristate area. And in 2018, Weiler Hospital launched an emergency department (ED) hospitalist program, conceived by Dr. Southern, in which ED-based hospitalists care for patients who are waiting to be admitted to a medicine unit.
“This frees up ED physicians to focus on treating patients truly in need of emergency care,” says Tulay Aksoy, M.D., assistant professor of medicine at Einstein and a hospitalist at Montefiore, who led the program at its inception.
“By the time patients are moved to the ward, we’ve already prepped them for admission,” she says. She notes that the program has also helped expand the ED’s capacity and reduced the length of inpatient hospital stays.
 Jessica Dekhtyar, M.D., right, and patient-care coordinator Renee Wehner-Dryden, R.N., discuss the transfer of acutely ill patients from satellite hospitals to Monefiore's Moses campus.
Jessica Dekhtyar, M.D., right, and patient-care coordinator Renee Wehner-Dryden, R.N., discuss the transfer of acutely ill patients from satellite hospitals to Monefiore's Moses campus.
Dr. Southern likes to tell a story about what hospitalists offer their patients. In early 2018, a 76-year-old man was admitted to Montefiore in the last throes of lung cancer. His daughter planned to get married at the end of the year and was concerned that he probably wouldn’t live long enough to walk her down the aisle.
When the man’s hospitalist, Zsuzsanna Sidlo, M.D., assistant professor of medicine at Einstein, learned of his daughter’s worry, she arranged to have a mini–wedding ceremony that very day in the patient’s room, and she gathered her unit’s staff to bear witness.
“Needless to say, there were a lot of tears in the room,” Dr. Southern says. “A few days later, the patient was transferred to Calvary Hospital, where he passed away peacefully within a week.”
The original version of this article did not include the fact that pediatric hospital medicine has been recognized since 2015 as a board-certified specialty.